Download
1 / 47
470 likes | 549 Views
High rates of HIV infection in the absence of greater risk among Black MSM. Greg Millett Centers for Disease Control Division of HIV/AIDS Prevention.

E N D
High rates of HIV infection in the absence of greater risk among Black MSM Greg Millett Centers for Disease Control Division of HIV/AIDS Prevention The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention
Race/ethnicity of MSM Diagnosed with HIV, 2005 1% 19% 32% 46% Source: Centers for Disease Control and Prevention. “HIV/AIDS among Men who have Sex with Men.” Fact Sheet. June 2007.
HIV Diagnoses by Age HIV Dx among MSM ages 13-24 • (MMWR, 2001; MWWR, 2005)
HIV Diagnosis & AIDS Mortality Diagnosed later in infection (Wortley et al., 1995) Quicker disease progression (Blair et al., 2002; Hall et al., 2007) Mortality (era after HAART) • 1996-1998 (Blair et al., 1995) • 1996-2002 (Hall et al., 2007)
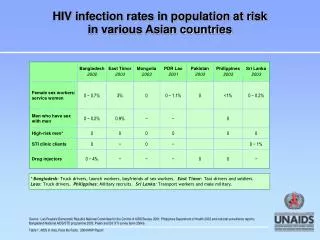
Gonorrhea, Chlamydia, Syphilis and HIV among men who have sex with men, byrace/ethnicity, STD clinics, 2005 • *Excludes persons previously known to be HIV-positive. • Seroreactivity.
HIV/STD Coinfection • Among 4000 MSM tested between 1990 and 1999 in NYC (Torian et al., 2002) • HIV+ Black MSM more likely than HIV+ White MSM to be coinfected with Gc, syphilis or nongonococcal urethritis (60% vs. 18%)
HIV M-to-F Transgender Meta-anlysis • Analysis of 29 studies and 2700 transgender individuals (Herbst et al., 2007) • Overall HIV seropositivity 28%
HIV M-to-F Transgender Meta-anlysis • Analysis of 29 studies and 2700 transgender individuals (Herbst et al., 2007) • Overall HIV seropositivity 28% • By race/ethnicity • Latinos 16% • White 17% • Black 56%
Does individual risk behavior drive the epidemic among Black MSM?
Unprotected anal intercourse • Substance use (during sex and/or injection) • Crack/ Cocaine • Heroin • Poppers • Meth
Research Paradox “established risk factors for HIV infection in homosexual/ bisexual men do not explain the differences in HIV seroprevalence or seroconversion rates between blacks and whites.” Samuel et al., 1987
NHBS Amphetamine Use (past 12 mos) Data collection 2003 -2005 (17 MSAs) (n = 4510) (n = 2680) (n = 1739) (n = 449)
ByH Meth Use (Past 3 mos) Data collection 2005 -2006 (3 cities) n=1014 n=1148
Young MSM (ages 15-22): Substance Use Behavior (Harawa et al., 2004) *P< .05
Substance Use Across 20 Studies Compared with Black MSM, White MSM across studies: • 3 times more likely to use amyl nitrites • 54% more likely to use drugs associated with HIV infection (IDU, amphetamines, crack/cocaine, needle sharing, opiates, nitrites) • 40% more likely to use any illegal substance (Millett et al., 2007)
Young MSM (ages 15-22): Sexual Risk Behavior Yet compared with White MSM in this sample: Black MSM were 9 times more likely to be HIV-positive (Harawa et al., 2004) *P< .05
NHBS: Sexual Risk (ages18-81) n= 4510 n= 2680 n= 1739 (CDC, 2006)
NHBS: HIV Prevalence by Race (MMWR, 2005)
Unprotected Anal Intercourse Across 17 Studies • Comparable rates of UAI by time period • Comparable rates of receptive UAI • Comparable rates of UAI with ‘known’ HIV-positive partners • Comparable rates of sex trade (Millett, 2007)
What does (and does not) place Black MSM at risk for HIV infection?
Social/ Structural Interpersonal/ Network Individual
Black MSM 70% less likely to identify as gay(Millett, 2007) 60% less likely to disclose sexuality(Millett, 2007) Less likely to join gay org or read gay media(McKirnan, 1995; Stokes, 1996; Kennamer, 2000) Sexual risk with male partners and HIV prevalence is higher among gay ID men compared with nongay-ID (Wood, 1993; Pathela, 2006) Sexual risk with male partners and HIV prevalence is greater among disclosing rather than nondisclosing MSM (CDC, 2003) HIV infection by sexual identity 1100 Black MSM Bisexual men 76% less likely Heterosexual men 91% less likely(Millett, 2007) Individual-LevelDemographic Factors: Gay ID/ Disclosure
Individual-LevelDemographic Factors: Undiagnosed HIV • Greater rates among Black and Latino MSM • Ages 15-22: Black 91%, Latino 69%, White 60% (MacKellar et al., 2005) • Ages 18-81: Black 67%, Latino 48%, White 23% (CDC, 2005) • Known positives engage in fewer sexual risk behaviors with negative or unknown status partners (Colfax et al., 2002) • People with unrecognized infection primarily responsible for ongoing epidemic (Marks et al, 2006)
Individual-Level Psychological Factors: Abuse, Distress • History of sexual abuse associated with sexual risk (Fields, 2007; Wheeler, 2007) • Depressive distress associated with greater rates of sexual risk (Crawford, 2002; Myers, 2003)
CCR5 base 32 allele Protective against HIV infection (Marmor, 2001; Stephenson, 2001) Slower disease progression (Huang, 1996; Michael, 1997) <.1% of non-Whites (Martinson, 2000) Few studies of MSM and none of MSM of color (Millett, 2006) STI Increases risk of HIV infection or transmission (Flemming, 1999): Meta-analysis(Millett, 2007): Black MSM 2x more likely to be dx with a current STD 50% more likely to have GC 2x more likely to have syphilis Individual-LevelBiological Factors: Immunogenetics and STI
Individual-LevelBiological Factors: Circumcision • General population • Prevalence: White (81-88%), Black (65-73%), Latinos (42-54%)(Xu, 2007; Laumann, 1997) • MSM • Protects insertive partner only • 1 US examined circumcision among Black MSM. No association among (Millett, 2007) • Black MSM • Black MSM-only • Black MSM/W • Black MSM who reported only being tops
Negative peer norms toward condom use associated with greater rates of UAI (Bakeman, 2007; Jones, 2007; Hart & Peterson, 2004; Peterson, 1995) Gay ID associated with negative peer norms toward condom use and safer sex communication (Jones, 2007) Interpersonal Level: Communication/ Peer norms
Negative peer norms toward condom use associated with greater rates of UAI (Bakeman, 2007; Jones, 2007; Hart & Peterson, 2004) Gay ID associated with negative peer norms toward condom use and safer sex communication (Jones, 2007) Interpersonal Level: Communication/ Peer norms Sex with older male partners(Bingham, 2003) Intraracial sexual mixing(Bingham, 2003; CDC, 2003)
Interpersonal Level: Social Support/ Partner status • Social support: • Lower levels of social support associated with greater risk taking (Peterson, 1992) • Inverse relationship between social support and sexual risk among HIV-positive Black MSM (Ostrow, 1991) • Main vs. casual partner • Men with a main partner more likely to engage in insertive or receptive sex (Hart & Peterson, 2004)
Social/Structural Level:Poverty/ Healthcare • Poverty • Black MSM: Lower income associated with greater likelihood of HIV infection (Peterson, 1992; Mays, 1995) • Healthcare access/ utilization • Access: No differences in health insurance (Halkitis, 2003; Kass, 1999) • Utilization: HIV-positive Black MSM 57% less likely to access ART compared with HIV-positive White MSM (Millett, 2007) • Adherence: Less likely to adhere to meds (Kleeberger, 2001 & 2004)
Social/ Structural: Gay-related Development and Early Abuse ,,,, (Friedman, 2007)
Social/ Structural: Gay-related Development and Early Abuse ,,,, (Friedman, 2007) • Men who reported earlygay-related development were more likely to report • Harassment for being gay during childhood and adolescence • Sexual abuse (> once) during childhood and adolescence
Social/ Structural: Gay-related Development and Adult Health Outcomes (Friedman, 2007)
Social/Structural Level:Discrimination • History of discrimination associated with greater sexual risk (Zamboni, 2006) • Relationship also mediated by psychiatric symptoms
Traditional risk factors for HIV infection (UAI, substance use) are not similar for Black MSM and other MSM • Must address structural and interpersonal factors since individual risk does not explain HIV disparities among Black MSM
Create new behavioral interventions specific to Black MSM • Must partner with communities • Tailor existing effective behavioral interventions for MSM for Black MSM populations • Black MSM are not homogenous (i.e. drug use by coast, multiethnic vs not) • Investigate applicable biological interventions (PrEP, rectal microbicides, etc)
Encourage frequent HIV/STI screening (every 6 mos) • Link HIV-positive MSM (especially Black MSM) with appropriate care • Target gay-identified, ‘out’ men, MSM
Support men throughout their lifetime, not just when they are young • Focus on the whole person • Operate from an ‘asset’ rather a ‘deficit’ model (resiliency)
Amphetamine use (past 5 years) Black MSM: East vs. West Coast (n = 472) (n = 2202) (Sullivan, 1998)
YMS: Meth Use (Lifetime) Black MSM vs. Mixed MSM (n = 814) (n = 201) (Harawa, 2004)
YMS: Black vs. Multi-ethnic (Harawa, 2004)