Download
1 / 55
1.2k likes | 5.67k Views
Cryptosporidium. infects several persons infected with HIV early diagnosis and effective hygienic measures reduce infections and prolong life

E N D
Cryptosporidium Dr.T.V.Rao MD
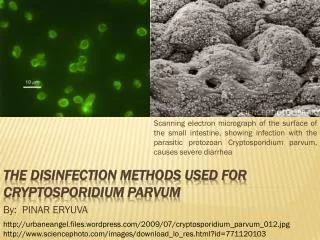
Cryptosporidiosis • Cryptosporidiosis, also known as crypto, is a parasitic disease caused by Cryptosporidium, a protozoan parasite in the phylum Apicomplexa. It affects the intestines of mammals and is typically an acute short-term infection. It is spread through the fecal-oral route, often through contaminated water, the main symptom is self-limiting diarrhea in people with intact immune systems. In immunocompromised individuals, such as AIDS patients,
Cryptosporidium • Cryptosporidium is a coccidian protozoan parasite that has gained much attention in the last 20 years as a clinically important human pathogen. The discovery of Cryptosporidium is usually associated with E.E. Tyzzer, who, in 1907, described a cell-associated organism in the gastric mucosa of mice (Keusch, et al., 1995). For several decades, Cryptosporidium was thought to be a rare, opportunistic animal pathogen.
First Human Infection with Cryptosporidiosis • But the first case of human cryptosporidiosis in 1976 involved a 3-year-old girl from rural Tennessee who suffered severe gastroenteritis for two weeks (Flanigan and Soave, 1993 )
Geographic Distribution: • Since the first reports of human cases in 1976, Cryptosporidium has been found worldwide. Outbreaks of cryptosporidiosis have been reported in several countries, the most remarkable being a waterborne outbreak in Milwaukee (Wisconsin) in 1993, that affected more than 400,000 people.
Parasite Survives in spite of Chlorine treatment • Many species of Cryptosporidium exist that infect humans and a wide range of animals. The parasite is protected by an outer shell that allows it to survive outside the body for long periods of time and makes it very resistant to chlorine disinfection.
Predisposed with ImmunodeficiencyAIDS a major concern • In the early 1980s, the strong association between cases of cryptosporidiosis and Immunodeficient individuals (such as those with AIDS--acquired immunodeficiency syndrome) brought Cryptosporidium to the forefront as a ubiquitous human pathogen.
Cryptosporidium Unique features, Caveats • Highly infectious • Transmitted through water, food, animal-to-human and human-to-human contact • Special precautions should be taken to prevent exposure: people with HIV and a CD4<200 should boil tap water for at least 1 minute to reduce risk of ingestion of oocysts in potentially contaminated drinking water. • May be the AIDS-defining presentation in patients who previously had few symptoms of HIV infection
Mode of infection • Swallowing or putting something contaminated with cryptosporidium into your mouth • Drinking water contaminated with cryptosporidium • Swimming in water contaminated with cryptosporidium and accidentally swallowing some of it • Eating uncooked food contaminated with cryptosporidium • Touching your hand to your mouth if your hand has been in contact with a contaminated surface or object • Having close contact with other infected persons.
Day care centers can spread the infection • Cryptosporidium transmission occurs at a high frequency in day-care centres, where infants or younger children are clustered within classrooms, share toilets and common play areas, or necessitate frequent diaper-changing (Keusch, et al., 1995).
Risk factors • Those who are exposed to contaminated water • Children, particularly those in diapers, who attend child care centres • Parents of infected children • Child care workers • Animal handlers • Those who engage in oral-to-anal sexual activity
Risk factors • International travellers, especially those travelling to developing countries • Backpackers, hikers and campers who drink untreated, unfiltered water • Swimmers who swallow water in pools, lakes and rivers • People who drink water from shallow, unprotected wells
Cryptosporidium cysts are hard to destroy • Cryptosporidium can infect several different hosts, can survive most environments for long periods of time due to its "hardy cyst" (Keusch, et al., 1995), and inhabits all climates and locales.):
Cryptosporidium can infect other Organs • While the small intestine is the site most commonly affected, symptomatic Cryptosporidium infections have also been found in other organs including other digestive tract organs, the lungs, and possibly conjunctivitis
Infection with Cryptosporidium sp cause • Infection with Cryptosporidium sp. results in a wide range of manifestations, from asymptomatic infections to severe, life-threatening illness; incubation period is an average of 7 days (but can range from 2 to 10 days). Watery diarrhea is the most frequent symptom, and can be accompanied by dehydration, weight loss, abdominal pain, fever, nausea and vomiting.
Molecular typing characterizes several species • The use of molecular tools in epidemiologic investigations has provided new insights into the diversity of Cryptosporidium spp. infecting humans and animals . There are at least 16 established Cryptosporidium spp. and >40 unnamed genotypes that are potentially different species..
Several species of Cryptosporidium infects humans • At least 8 of them have been reported in humans: C. hominis, C. parvum*, C. meleagridis, C. felis, C. canis,C. muris, and C.suis, and the Cryptosporidium cervine genotypes. *Most common infecting species
Life Cycle • 1 Excystation of the orally ingested oocyst in the small bowel with release of the four sporozoites • 2 Invastion of intestinal epithelial cells via the differentiated apical end of the sporozoite within a vacuole formed of both host and parasite membranes and the initiation of the asexual intracellular multiplication stage
Life Cycle • 3 Differentiation of microgamete's and macrogamete's • 4 Fertilization initiating sexual replication • 5 Development of oocysts • 6 The formation of new, infectious sporozoites within the oocyst, which is then excreted in the stool
Immunocompetence makes the difference in severity of Infections • In immunocompetent persons, symptoms are usually short lived (1 to 2 weeks); they can be chronic and more severe in immunocompromised patients, especially those with CD4 counts <200/µl
Cryptosporidium can hitch a ride on food-or in water-causing diarrhea and even death in vulnerable individuals.
Cryptosporidium parvum & hominis – Life cycle Thin-walled Thick-walled Auto- Infective Cycle
Manifest in Immunocompetent patients with , • Frequent, watery diarrhea • Nausea • Vomiting • Abdominal cramps • Low-grade fever (In immunocompetent patients, cryptosporidiosis is an acute, yet self-limiting diarrheal illness (1-2 week duration), and symptoms include (Juranek, 1995):
In immunocompromised persons • Debilitating, cholera-like diarrhea (up to 20 liters/day) • Severe abdominal cramps • Malaise • Low-grade fever • Weight loss • Anorexia In immunocompromised persons, the illness is much more severe (Juranek, 1995):
Laboratory Diagnosis: • Acid-fast staining methods, with or without stool concentration, are most frequently used in clinical laboratories. For greatest sensitivity and specificity, immunofluorescence microscopy is the method of choice • Molecular methods are mainly a research tool.
Safety in handling Stool specimens • Oocysts in stool specimens (fresh or in storage media) remain infective for extended periods. Thus stool specimens should be preserved in 10% buffered formalin or sodium acetate-acetic acid-formalin (SAF) to render oocysts nonviable. The usual safety measures for handling potentially infectious material should be adopted.
Processing of Stool specimens • Stool specimens may be submitted fresh, preserved in 10% buffered formalin (see above, “Safety”), or suspended in a storage medium composed of aqueous potassium dichromate (2.5% w/v, final concentration). • Multiple stool samples should be tested before a negative diagnostic interpretation is reported. To maximize recovery of oocysts, stool samples should be concentrated prior to microscopic examination.
Shortcomings of oocyst concentration techniques are: • Sedimentation methods are generally performed using low speed centrifugation. Given their small size and mass, cryptosporidial oocysts may become trapped in the ether or ethyl acetate plug and fail to sediment properly. Increased centrifugation speed or time (500 × g, 10 minutes) may be warranted when attempting to recover cryptosporidial oocysts. • Resolution of cryptosporidial infections is accompanied by increasing numbers of non-acid-fast, oocyst “ghosts.” Such oocysts may not float or sediment as expected, giving rise tofalse-negative results.
Modified Kinyoun’s Acid-Fast Stain (cold) Protocol • Smear 1 to 2 drops of specimen on the slide, and allow it to air dry. Do not make the smears too thick (you should be able to see through the wet material before it dries). Prepare two smears. • 2. Fix with absolute methanol for 1 min. • 3. Flood slide with Kinyoun’s carbol fuchsin, and stain for 5 min. • 4. Rinse slide briefly (3 to 5 s) with 50% ethanol
Modified Kinyoun’s Acid-Fast Stain(cold) Protocol (Cont) • 5. Rinse thoroughly with water. • 6. Decolorize with 1% sulfuric acid for 2 min or until no more colour runs • from the slide. • 7. Rinse slide with water. Drain. • 8. Counter stain with methylene blue or brilliant green for 1 min. • 9. Rinse slide with water. Air dry. • 10.Examine using low or high dry objectives. To see internal morphology, • Use oil objective (100X).
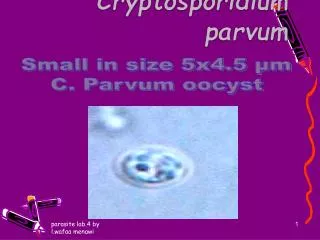
Modified acid-fast stain • Oocysts (4 to 6 μm) often have distinct oocyst walls and stain from light pink to bright red. However, staining may be variable. In particular, infections that are resolving can have colourless oocyst “ghosts.” Mature oocysts may have discernible sporozoites
Direct fluorescent antibody (DFA) assay • This technique offers the highest combination of sensitivity and specificity and is considered the gold standard by many laboratories. However, it does not provide a stained slide that can be archived.
Other methods for detecting Cryptosporidium in stool. • Enzyme immunoassay (EIA)The EIA does not rely on microscopy skills, is highly sensitive and specific, and is useful for screening large numbers of specimens. Rapid immunochromatographic cartridge assays The rapid cartridge assays may be used with preserved specimens and are quick and easy to perfor
Antibody Detection for Epidemiological studies • Antibody detection: There are currently no commercially available serologic assays for the detection of Cryptosporidium-specific antibodies. However, immunoblots for detecting the 17 and 27 kDa sporozoite antigens associated with recent infection may be useful for epidemiologic investigations.
Genetic methods in Diagnosis • Genetic methods for detecting oocysts have been developed that identify and amplify Cryptosporidium nucleic acids using the Polymerase Chain Reaction (Johnson, et al., 1995). Oocysts were detected by PCR in wastewater, surface waters, and drinking water, but the sensitivity of the PCR assay was inhibited by "uncharacterized components in the samples."
Real-Time PCR • TaqMan-based real-time PCR assay for detection and speciation of Cryptosporidium parvum (bovine genotype) and Cryptosporidium hominis (human genotype) has been developed and validated at CDC. The assay combines the detection of two genomic targets: the 18S rRNA gene to achieve a sensitive detection of Cryptosporidium spp. and a gene with unknown function to provide species differentiation.
Out Breaks with Cryptosporidium • Drinking from contaminated public water supplies • Drinking unpasteurized cider • Swimming in contaminated pools and lakes
Drinking water and Cryptosporidium • Drinking water: In recent years there has been increasing recognition of outbreaks of cryptosporidiosis arising from contamination of water supplies. Although resistant to many chemical disinfectants, including chlorine used to treat water, properly functioning water treatment systems are usually able to deal with the small numbers of oocysts which are present from time to time in water sources such as rivers.
Hand Washing is most affordable precaution • Wash your hands with soap and warm water often. Do this before preparing meals and after going to the bathroom, changing diapers, or handling pets. Teach your child to do the same.
Oral rehydration is minimal essential treatment • Since cryptosporidiosis is a self-limiting illness in immunocompetent individuals, general, supportive care is the only treatment for the illness. Oral or intravenous rehydration and replacement of electrolytes may be necessary for particularly voluminous, watery diarrhea.)
Oral rehydration treatment • Oral rehydration treatment can include oral rehydration solution, containing glucose, sodium bicarbonate, and potassium (Flanigan and Soave, 1993)
Guidelines as per CDC • Outbreaks of cryptosporidiosis have been linked to municipal water supplies. During outbreaks or in other situations in which a community advisory to boil water is issued, boiling water for 1 minute will eliminate the risk for cryptosporidiosis. Using submicron personal-use water filters† (home/office types) or bottled water§ also might reduce the risk.
Should HIV patients should boil the water ? CDC • The magnitude of the risk for acquiring cryptosporidiosis from drinking water in a nonoutbreak setting is uncertain, and available data are inadequate to recommend that all HIV-infected persons boil water or avoid drinking tap water in nonoutbreak settings
HIV infected should avoid - CDC ….. • HIV-infected persons should avoid eating raw oysters because cryptosporidial oocysts can survive in oysters for >2 months and have been found in oysters taken from certain commercial oyster beds .
HIV infected should avoidCDC … • Cryptosporidium-infected patients should not work as food handlers, including if the food to be handled is intended to be eaten without cooking. Because the majority of food borne outbreaks of cryptosporidiosis are believed to have been caused by infected food handlers,
Hand Washing a great concern in HIV infected – can prolong life