Download

1 / 19
190 likes | 421 Views
By: Dr. Josh Funk, DPT, CSCS Founder of Lax Factory Physical Therapist. Power Development for Rotational Sport Athletes. Power Development is Plane-Specific!. About the Speaker. Maryland native Multi-sport athlete growing up College Lacrosse at Ohio State Professional Lacrosse in the NLL

E N D
By: Dr. Josh Funk, DPT, CSCS Founder of Lax Factory Physical Therapist Power Development for Rotational Sport Athletes Power Development is Plane-Specific!
About the Speaker • Maryland native • Multi-sport athlete growing up • College Lacrosse at Ohio State • Professional Lacrosse in the NLL • Doctor of Physical Therapy at the University of Maryland • Wearing many hats as a sport coach, performance coach and physical therapist
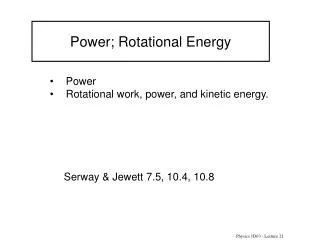
What is Power? • Noun • Physical strength and force exerted by something or someone • Verb • To move or travel with great speed or force • How do I train carryover?
Anecdotal • MPH correlation with medicine ball toss and lateral bounds • Ages 10-17 • 6 kg med ball • 3 reps each side • Correlation on dominant hand • Non-dominant hand affected by technique errors • Grip strength also correlated
Current Concepts • Most research performed in baseball world • Improving sagittal plane performance markers is not correlated with increased throwing velocity • Ground reaction forces must be trained in the direction of the skill at hand • Power Development is plane specific • Increased levels of force production in back leg leads to higher throwing velocity • Increased stride length leads to increased power • Postural Restoration Institute
Asymmetrical Brain and Body • Liver on 1 side • 3 lobes of lung on R vs 2 on L • Diaphragm attachments more expanside on R • R diaphragm built for success • More common to see L rib flares • In addition to hard wiring making most of us left brain dominant for certain motor tasks Courtesy of Postural Restoration Institute
Balancing Asymmetries • L AIC • L Psoas • R Diaphragm • L TFL • L VastusLateralis • R Biceps Femoris • R IC Adductors • R BC • R Diaphragm • R Oblique • L Pec • R TriangularisSterni • PEC • Superficial Back Extensors • Janda Lower Crossed
Program Considerations • Left versus Right Handed Athlete • In-Season vs Off-Season • Pre-Season vs. Off-Season • Weight of the Medicine Ball (Strength-Speed) • Injury History • Sport and Position of the Athlete • Elasticity of the Athlete • Postural Restoration Institute
What We Do • PRI themed Activation • Dynamic Flexibility • Frontal (bands) and Transverse plane bounds Medicine Ball Throws • Frontal Plane and Single Leg Strength Training • Anti-Movements • Sled Dragging
Why Medicine Balls? • Teach total body power development • Allow you to safely load athlete’s in the sagittal, frontal and transverse planes • Can reinforce ankle, hip and T-spine mobility • Able to train the Strength-Speed portion of the training continuum • Can reduce acquired asymmetries • Stress reducer • FUN!!!
Cues for Medicine Ball • “Load To Explode” • Forearm parallel to the ground • Pull elbow back to the wall behind you • Back of front shoulder should face the target • Off hand support • Emphasis on Loading the back leg • “Push off” after you weight shift to back leg • “Cover Ground”- Get as close to the wall as possible after you throw • “Get Long” Full extension of the hands and arms • Don’t allow back leg to be “Stuck in the Mud”
Medicine Ball Progressions • Without Stretch-Shortening Cycle (SSC) • With Stretch-Shortening Cycle • Exaggerated Stretch Component • Can Vary: • Amplitude • Short • Long • Response • Short • Long • REMEMBER- Power Development is Plane Specific!!!
Medicine Ball Variations • Linear • Granny Toss to Chest Pass to Overhead • Lateral/Rotational • Scoop Toss to Mid Rotational Toss to Shot Put • Stance Variations • Tall Kneel to Half Kneel • Symmetrical to Asymmetrical Stance • Stepping to Footwork
Medicine Ball Footwork • Stationary • Stepping • Jump, Leap and Hop • Locomotion • Shuffle • Carioca • Skipping • Skipioca • Possibilities are endless
Anti-Movements • Can Use Partner for Iso’s • If solo, perform press-outs • Positions • Half Kneel (In-line or regular) • Tall Kneel • Iso Split Squat • Athletic Position • Quadruped • Chops and Lifts • Y-Balance Reach • Usually use as A2 or A3 during weight program
Additional Emphasis • Landing on 1 leg • Eccentric strength on the lead leg is equally as important • Need for bowler squats, single leg deadlifts, lateral lunge variations, etc. • Can train eccentric for lead leg with medicine balls (should always)
References • MacWilliams, B, Choi, T, Perezous, M, Chao, E, and McFarland, E. Characteristic ground reaction forces in baseball pitches. Am J Sports Med 26: 66-71, 1998. • Matsuo, T, Escamilla, R, Fleisig, G, Barrentine, S, and Andrews, J. Comparison of kinematic and temporal parameters between different pitch velocity groups. J ApplBiomech 17: 1-13, 2001. • Spaniol, FJ. Predicting throwing velocity in college baseball players. J Strength Cond Res 11: 286, 1997. • Lehman G, Drinkwater, ER, Behm, DG. Correlation of throwing velocity to the results of lower-body field tests in male college baseball players
Medicine Ball Madness DEMO!
Thank you! • Dynamax • Mike Boyle • Charlie Weingroff • Eric Cressey • Kevin Neeld • Kyle Tarp • Dave Gottfeld • Ron Hruska • Rob Taylor