Download
1 / 1
10 likes | 140 Views
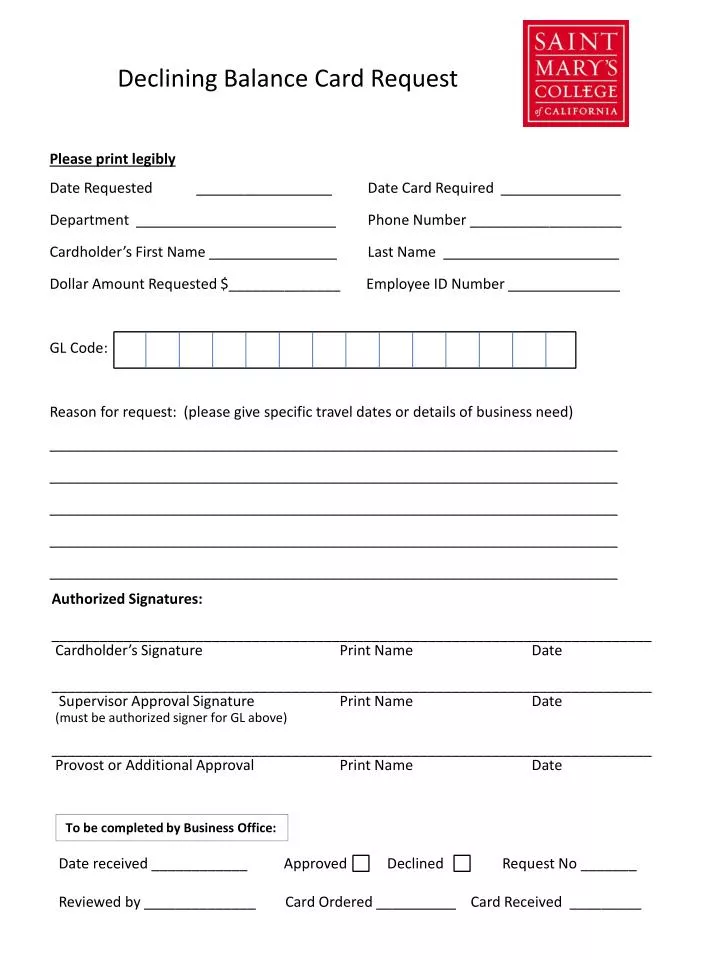
Declining Balance Card Request. Date Requested _________________ Date Card Required _______________ Department _________________________ Phone Number ___________________ Cardholder’s First Name ________________ Last Name ______________________

E N D
Declining Balance Card Request Date Requested _________________ Date Card Required _______________ Department _________________________ Phone Number ___________________ Cardholder’s First Name ________________ Last Name ______________________ Dollar Amount Requested $______________ Employee ID Number ______________ GL Code: Reason for request: (please give specific travel dates or details of business need) _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ Please print legibly Authorized Signatures: ___________________________________________________________________________ Cardholder’s Signature Print Name Date ___________________________________________________________________________ Supervisor Approval Signature Print Name Date (must be authorized signer for GL above) ___________________________________________________________________________ Provost or Additional Approval Print Name Date To be completed by Business Office: Date received ____________ Approved Declined Request No _______ Reviewed by ______________ Card Ordered __________ Card Received _________