Download
1 / 1

E N D
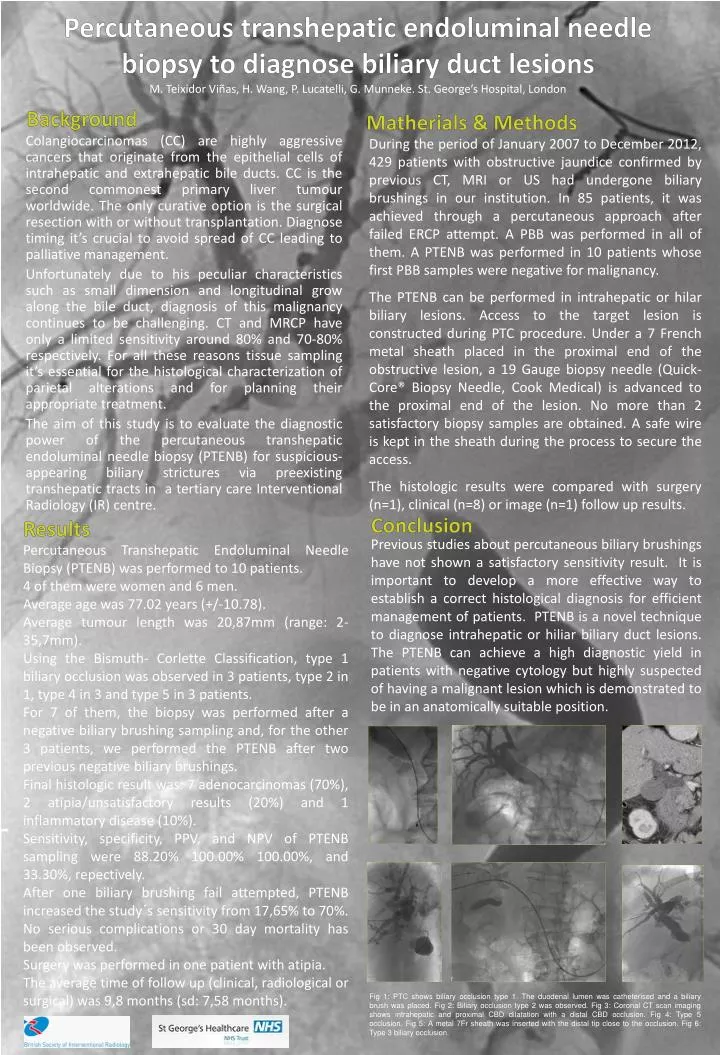
Background Matherials & Methods During the period of January 2007 to December 2012, 429 patients with obstructive jaundice confirmed by previous CT, MRI or US had undergone biliary brushings in our institution. In 85 patients, it was achieved through a percutaneous approach after failed ERCP attempt. A PBB was performed in all of them. A PTENB was performed in 10 patients whose first PBB samples were negative for malignancy. The PTENB can be performed in intrahepatic or hilar biliary lesions. Access to the target lesion is constructed during PTC procedure. Under a 7 French metal sheath placed in the proximal end of the obstructive lesion, a 19 Gauge biopsy needle (Quick- Core® Biopsy Needle, Cook Medical) is advanced to the proximal end of the lesion. No more than 2 satisfactory biopsy samples are obtained. A safe wire is kept in the sheath during the process to secure the access. The histologic results were compared with surgery (n=1), clinical (n=8) or image (n=1) follow up results. Percutaneous transhepaticendoluminal needle biopsy to diagnose biliary duct lesionsM. TeixidorViñas, H. Wang, P. Lucatelli, G. Munneke. St. George’s Hospital, London Conclusion Results Previous studies about percutaneous biliary brushings have not shown a satisfactory sensitivity result. It is important to develop a more effective way to establish a correct histological diagnosis for efficient management of patients. PTENB is a novel technique to diagnose intrahepatic or hiliar biliary duct lesions. The PTENB can achieve a high diagnostic yield in patients with negative cytology but highly suspected of having a malignant lesion which is demonstrated to be in an anatomically suitable position. Percutaneous Transhepatic Endoluminal Needle Biopsy (PTENB) was performed to 10 patients. 4 of them were women and 6 men. Average age was 77.02 years (+/-10.78). Average tumour length was 20,87mm (range: 2-35,7mm). Using the Bismuth- Corlette Classification, type 1 biliary occlusion was observed in 3 patients, type 2 in 1, type 4 in 3 and type 5 in 3 patients. For 7 of them, the biopsy was performed after a negative biliary brushing sampling and, for the other 3 patients, we performed the PTENB after two previous negative biliary brushings. Final histologic result was: 7 adenocarcinomas (70%), 2 atipia/unsatisfactory results (20%) and 1 inflammatory disease (10%). Sensitivity, specificity, PPV, and NPV of PTENB sampling were 88.20% 100.00% 100.00%, and 33.30%, repectively. After one biliary brushing fail attempted, PTENB increased the study´s sensitivity from 17,65% to 70%. No serious complications or 30 day mortality has been observed. Surgery was performed in one patient with atipia. The average time of follow up (clinical, radiological or surgical) was 9,8 months (sd: 7,58 months). Colangiocarcinomas (CC) are highly aggressive cancers that originate from the epithelial cells of intrahepatic and extrahepatic bile ducts. CC is the second commonest primary liver tumour worldwide. The only curative option is the surgical resection with or without transplantation. Diagnose timing it’s crucial to avoid spread of CC leading to palliative management. Unfortunately due to his peculiar characteristics such as small dimension and longitudinal grow along the bile duct, diagnosis of this malignancy continues to be challenging. CT and MRCP have only a limited sensitivity around 80% and 70-80% respectively. For all these reasons tissue sampling it’s essential for the histological characterization of parietal alterations and for planning their appropriate treatment. The aim of this study is to evaluate the diagnostic power of the percutaneous transhepatic endoluminal needle biopsy (PTENB) for suspicious-appearing biliary strictures via preexisting transhepatic tracts in a tertiary care Interventional Radiology (IR) centre. Fig 1: PTC shows biliary occlusion type 1. The duodenal lumen was catheterised and a biliary brush was placed. Fig 2: Biliary occlusion type 2 was observed. Fig 3: Coronal CT scan imaging shows intrahepatic and proximal CBD dilatation with a distal CBD occlusion. Fig 4: Type 5 occlusion. Fig 5: A metal 7Fr sheath was inserted with the distal tip close to the occlusion. Fig 6: Type 3 biliary occlusion.






















