Download
1 / 49
500 likes | 1.02k Views
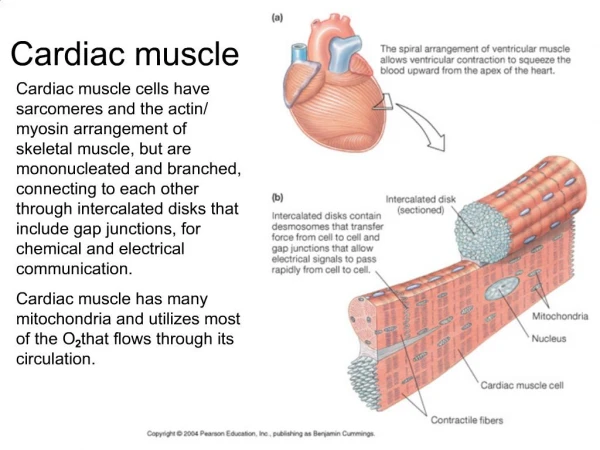
Striated like skeletal muscle. Myosin Actin Mitochondria. Cardiac Muscle is only found in the heart. II. Cardiac muscle Action Potentials A. Phase 0 due to opening of fast voltage-gated sodium channels. Potassium channels close at this time (there are many types of potassium channels).

E N D
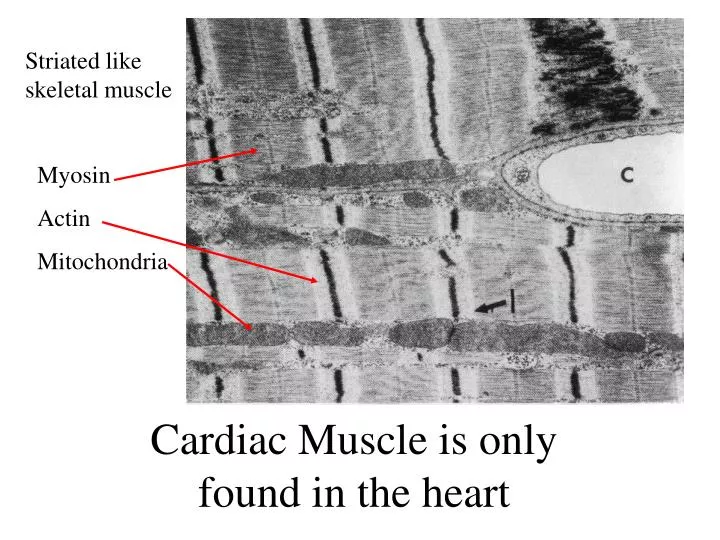
Striated likeskeletal muscle Myosin Actin Mitochondria Cardiac Muscle is only found in the heart
II. Cardiac muscle Action Potentials • A. Phase 0 due to opening of fast voltage-gated sodium channels. Potassium channels close at this time (there are many types of potassium channels). • Phase 1 due to brief opening of transient outward rectifier potassium channels (Ito) • Phase 2 is due to slow Calcium channels (L-type) • D. Phase 3 is due to reopening of the potassium channels and closure of calcium channels. • E Phase 4 the resting condition (Potassium channels stay open).
II. Cardiac muscle Action Potentials • The plateau phase is important because it keeps the actin / myosin molecules activated for 300 ms. That is long enough for the ventricle to eject its blood into the aorta. • The Ca++ that enters during that phase helps activate the muscle.
Specialized cardiac muscle types • All cardiac muscles have rhythm, conduction and contractility • Heart beat is myogenic (beat originates in the muscle) • There are different subtype of cardiac muscle that specialize in just one of the above properties
Membrane Voltage (mv) IV. Electrical properties of pacemaker cells in SA node A. Small cells 3-5u in diameter B. Sharp spike is absent (no fast Na+ channels) Phase 0 from slow Ca++ channels C. Pacemaker potential between APs D. Pacemaker potential is due to gradual drop in K+ conductance and and an increase in Na+ conductance “the funny current” (If).
A. Sympathetic nerves secrete norepinephrine and speed up the rate by increasing cAMP in the SA node. B. cAMP opens the hyperpolarization-activated cyclic nucleotide-gated (HCN) sodium channels which increases If (funny current) during phase 4. C. Question - How many pacemaker cells participate in each beat?
VI. Changing the rate of the cardiac pacemakers A. Two nerve populations –sympathetic & parasympathetic B. Parasympathetic (vagus) secrete acetylcholine and slow the heart rate C. Acetylcholine increases K+ conductance which hyperpolarizes the SA nodal cells. It also lowers cAMP by its Gi-coupling
Like skeletal muscle mechanical contraction lags behind the action potential.
Absolute refractory period: all inactivation gates are closed no electrical stimulus will elicit another action potential. Runs from phase 0 through most of phase 3. Because of the long refractory periods heart muscle cannot be tetanized. Relative refractory period: some inactivation gates are open. An action potential can be elicited but a higher stimulus voltage is required and not all channels participate.
II. Conduction • A. Action Potentials spread from cell to cell electrically. • 1. Depolarization causes ions in one cell to spread through gap junctions of the next triggering a second action potential Cytoplasm cell 1 Cytoplasm cell 2
II. Conduction • 2. Rate of spread through tissue determined by: • a. Diameter of fibers • b. Prevalence of gap junctions • c. Rate of rise of the action potential Ventricularmyocyte (slow) Purkinje (fast)
II. Conduction • 3. Safety factor: usually there is much more current generated by a cell than is required to stimulate its neighbor • 4. An action potential in any cell will spread over the entire heart
The heart beat originates in the SA node (the pacemaker) and spreads over the heart by cell to cell conduction through a complex pathway. Since many diseases affect conduction it is important to understand its complex route.
The SA node is the pacemaker because it has the fastest rhythm. It is the first structure to show electrical activity with each beat.
Purkinje fibers conduct fastest They are large diameter, have many gap junctions and fast phase 0.
AV Nodal tissue is slowest It has small diameter cells, few gap junctions and slow phase zero
Atrial , ventricular, and Bundle of His tissue conducts at about 1 m/sec
AV node is vulnerable to Injury from disease which can cause loss of conduction to the ventricles.(Heart block). The AV node is the only pathway to the ventricles The paucity of gap junctions in the AV node also causes a low safety factor (the amount of current passed to the next cell/the amount of current needed to reach threshold).
The slow conduction in the AV node causes the atria to contract before the ventricles which aids in ventricular filling. • The AV node’s long refractory period filters out high heart rates from atrium. • Some patients have an accessory bypass pathway with no delay between atrial and ventricular contraction. (Wolf, Parkinson, White or WPW) • D. WPW patients are vulnerable to atrial tachyarrhythmias like atrial fibrillation..
Ablation of the AV node slows the heart rate down to that of the next highest pacemaker Heart Block
Ablation of the fast-conducting tissue below the AV bundle is very serious since the spontaneous rate for Purkinje fibers is dangerously low.
As the heart beats action potentials on the heart cause an electrical signal on the body surface. The larger the structure the greater the voltage it induces. This voltage pattern is called the electrocardiogram
Conduction through the small AV node is associated with virtually no electrical signal on the skin.
QRS is large because the ventricular mass is large Depolarization of the ventricle causes the QRS complex. QRS is short because conduction over the ventricles is very fast
Repolarization of the ventricle causes the T wave Dispersion causes it to be smaller and last longer than the QRS complex. Repolarization is not a conducted wave.
Q wave; If the first deflection of the QRS complex following the P wave is negative then it is called a Q wave (may be absent)
R wave; the first positive deflection in the QRS complex (may be absent)
S wave; A negative deflection following an R wave (may be absent) If the voltage goes positive again after an S wave that is called an R’. If it goes negative again then that wave is called an S’.
Intervals are times and segments are voltages P-R interval; the time from the start of the P wave to the start of the QRS complex. (0.12-0.21 sec) - atrial conduction + AV node conduction + bundle of His conduction. Estimate of AV node conduction time.
If P-R interval is too long it means conduction in the AV node is depressed (First Degree Heart Block). If P-R interval is too short it indicates an accessory pathway of fast-conducting tissue is bypassing the AV node (WPW).
QRS interval (duration); 0.07 to 0.10 sec (time to depolarize entire ventricle). May be long in hypertrophied or failing ventricle.
Q-T interval; depolarization plus repolarization in the ventricle (from the first cell to depolarize to the last cell to repolarize). Estimate of AP duration. Some drugs extend the Q-T interval.
ST and PR segments; should be isoelectric (zero volts) in a normal EKG.
Rate = 1/ R-R interval (if you use times in seconds don’t forget to multiply by 60 for beats per minute) A shortcut: Rate = 1500 / # of small boxes in an RR interval
In a standard ECG, recordings are performed sequentially from 12 different positions on the body surface.
That produces 12 different ECG plots for each patient. Each of these will differ as to the magnitude and polarity of the voltages they record.
That is why some configurations may lack a Q wave while others may lack an R or S wave in the same individual.
All lead configurations will exhibit the same timing relative to the basic P wave, QRS complex, and T wave.
Heart Block: Depressed conduction through the AV node. A. first degree: slowed conduction (long PR interval)
Second degree: Intermittent conduction (dropped beats) • Mobitz I (variable P-R) • Mobitz II (no change in P-R)
Third degree: no conduction (atria and ventricles beat independently). Ventricles beat slowly to a ventricular pacemaker
In ventricular fibrillation the heart looses its coordinated beat and just quivers (sudden death).
Fast Sodium: Voltage-gated sodium channels. Cause rapid rise of phase zero in atrial, Purkinje, and ventricular cells. Not expressed in AV or SA nodal cells. Blocked by tetrodotoxin (puffer fish toxin). They are also responsible for action potentials on nerve and skeletal muscle. Potassium channels. There are many and they operate in a complex manner but essentially they increase their collective conductance during phase 3 and help restore the resting potential. One channel type, the transient outward rectifying channels (Ito), open briefly during phase 1 and are responsible for the brief fall in membrane potential at this time.
HCN (the hyperpolarization-activated cyclic nucleotide-gated) channels: These conduct sodium and are thought to be responsible for the “funny” current (If) that causes the progressive depolarization of the SA node cells during phase 4. Expressed in the nodal tissue. These belong to a class called cyclic nucleotide gated (CNG) channels because increasing cAMP in the cell opens the channel which increases heart rate. This is not in the textbook. KACh : These potassium channels are found it the atrium including the SA node. Gi alpha causes the channels to open and hyperpolarize the SA node thus slowing the heart rate. This is not in the textbook.