Download
1 / 59
590 likes | 731 Views
Historique accès ARV Génériques Recommandations OMS Discussions. Cours IMEA/Fournier 19/11/2006 Dr Roland Landman. Access to ARV in developing countries: pieces of History (1). 1981: First AIDS cases reported 1984: HIV discovery 1987: AZT licensed

E N D
Historique accès ARV • Génériques • Recommandations OMS • Discussions Cours IMEA/Fournier 19/11/2006 Dr Roland Landman
Access to ARV in developing countries: pieces of History (1) • 1981: First AIDS cases reported • 1984: HIV discovery • 1987: AZT licensed • 1990: 80 % reduction of MTC transmission with AZT during pregnancy + labor (IV) + 6-week newborn regimen • 1992: Superiority of Double Therapy vs Monotherapy • 1996: First HAART regimen (triple therapy including protase inhibitor) • 1997-1998: Major impact of HAART on AIDS morbidity & mortality
Access to ARV in developing countries: pieces of History (2) • 1993: Thailand starts producing AZT generics without publicizing • 1996: First mobilization for drug access to developing countries. Gay community claims for ARV in Brazil. • 1997: African AIDS conference (Abidjan), « Patients are in South, Drugs are in North » • 1998: « Bridging the Gap » (International AIDS Conf, Geneva) • 1998: Brazil starts producing generics • 1998: Sénégal launches National Access to Antiretrovirals; WHO creates with 5 companies the « Access program » with cut prices. • 1999: Activists and NGO claim access to ARV at WTO meeting (Seattle)
Access to ARV in developing countries: pieces of History (3) • 1999: Activists and NGO claim access to ARV at WTO meeting • (Seattle). GSK cuts AZT prices for MTC prevention. • 2000: G8 commits to facilitate ARV access to developing countries • 2000-2001: Major decrease of drug prices • Brazil offers to sell generics (« mandatory license ») • Cipla (India) offers triple therapy for $ 600/year instead of $ 600/month • Accelerated Initiaitive Access (UNAIDS) • 2001: Pretoria trails: 39 Drug Companies withdraw prosecution against developing countries govt • 2001: UN launches « Global Fund against AIDS, malaria & TB » • 2003: US pdt announces $ 15 billions against AIDS, malaria, TB
Why we want to introduce ARV in developing countries : a biosocial analysis (P. Farmer, 2002) • Because they are effective and will reduce suffering, mortality, HIV transmission ? • Because the transnational « outcome gap » is growing • Because HIV prevention may be re-enforced by attending to each of the above • Because they are demanded by those most affected by HIV
Reasons to treat AIDS in Africa (1) • Important component of a strategy to support people living with HIV and AIDS as well as preventing transmission of infection • People may be more willing to undergo voluntary counselling and testing • People may be more willing to disclose their HIV status if there is a possibility of getting effective treatment
Reasons to treat AIDS in Africa (2) • By reducing viral load , ARVs might also reduce the risk of sexual transmission • Sick people will be able to return to work. • Parents will stay alive longer, thus delaying the time when children become orphans • The rate of mother-to-child-transmission will be reduced
POPULATION OBJECTIVES OF ARV DRUG THERAPY PROGRAMS Objective 1: Maintaining Economic Stability Objective 2: Achieving Distributive Justice Objective 3: Curbing the HIV Epidemic Objective 4: Reducing Morbidity and Mortality Desvarieux et al. July 2005, Vol 95, No. 7 | American Journal of Public Health
Basic minimum package for HIV in endemic settings • Agressive AIDS prevention programmes, including barrier methods • Social assistance to HIV-affected families, including orphans • Maternal-child transmission package (including milk supplements) • Diagnosis, treatment and prevention of opportunistic infections and sexually transmitted diseases • Post-exposure prophylaxis for rape and professional accidents • HAART
Five key-elements for antiretroviral policy package 1-Government commitment 2-Case detection through passive case finding 3-Standardized antiretroviral regimens 4-Establishment of a regular drug supply 5-Establishment and maintenance of a monitoring system Harries AD et al Lancet 358, August 2001
Government commitment • Aim: scaling up • Integration with the national tuberculosis control programme • Package of care -Voluntary conselling and testing -Psychological support -Palliative care -Home based care -Essential drugs for the treatment and prevention of opportunistic infections and STD -Nutritional support
ARV in developing countries: main issues • Comprehensive programme re-enforcing prevention & VCT • MTCT prevention programme • Define eligibility criteria in the context of limited ressources • Ensure drug supplying and quality control • Define monitoring criteria: tolerance/efficacy
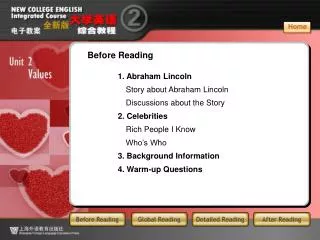
Estimated Number of HIV Infected Adults in Brazil in the Year 2000 Thousands 1400 1200 1000 50% 800 1,200,000 600 400 600,000 200 0 Brazilian MOH Estimate (2000) Word Bank Projection (1992) MOH, 2002
Historique accès ARV Génériques Recommandations OMS Discussions
Historique accès ARV Génériques Recommandations OMS Discussions
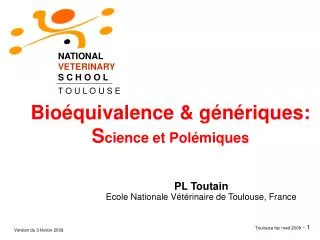
HAART limitations: lack of immune restoration against HIV HIV rebound when stopping HAART HAART Stop Immune responses against HIV HIV RNA / ml 4 8 years Ab, HIV killer cells CD4 anti-VIH Total CD4 HIV RNA
Presenting diagnoses in 200 patients with HIV disease, clinique Bon Sauveur (Haïti), 1993-95
G Grading of recommendations and levels of evidence Strength of recommendation, Level of evidence to make for recommendation A. A Recommended - should be followed B. B Consider - applicable in most situations C. C Optional I. I At least one randomized controlled trial with clinical, laboratory or programmatic endpoints II. II At least one high quality study or several adequate studies with clinical, laboratory or programmatic endpoints III. III Observational cohort data, one or more case controlled or analytic studies adequately conducted Ex IV Expert opinion based on evaluation of other evidence
Table 2 WHO classification of HIV-associated clinical disease a Classification of HIV-associated clinical disease WHO Clinical Stage Asymptomatic 1 Mild 2 Advanced 3 Severe 4 aAnnexes 1 and 2 provides further details on staging events and criteria for recognising them
Table 3 CD4 criteria for initiation of ART in Adults and Adolescents CD4 (cell /mm3) a Treatment recommendation b < 200 Treat irrespective of clinical stage c[A-III] 200 - 350 Consider treatment [B-III] and initiate ART before drop below 200 cell/mm3 c[A-III] >350 Defer treatment in asymptomatic persons [A-III] a CD4 cell count should be measured after stabilization of any intercurrent condition b CD4 cell count supplement clinical assessment and should therefore be used in combination with clinical staging in decision making c A drop of CD4 cell count below 200 cells/mm3 is associated with a significant increase of opportunistic infections and death
Table 4 Recommendations for initiating ART in adults and adolescents based on clinical stage and availability of immunological markers WHO Clinical Staging CD4 testing not available CD4 testing available 1 Do not treat [A-III] Treat if CD4 cell count < 200/mm3 a[A-III] 2 Do not treat c[B-III] 3 Treat[A-III] Treat irrespective of CD4 cell count, with consideration of CD4< 350/mm3 in some situations b[A-III] 4 Treat[A-III] Treat irrespective of CD4 cell count [A-III] a The precise CD4 cell level above 200/mm3 at which ARV treatment should be started has not been established. b CD4 cell count advisable to assist with determining need for immediate therapy for situations as pulmonary TB and severe bacterial infections, which may occur at any CD4 level. c A total lymphocyte count of ≤ 1200/mm3 can be substituted for the CD4 count when the latter is unavailable and mild HIV disease exist. It is not useful in the asymptomatic patients. Thus, in the absence of CD4 cell count and TLC, patients with WHO Adult Clinical Stage 2 should not be treated.
Table 8 Clinical, CD4 Cell Count, and Virological Definitions of Treatment Failure for Patients on a First-Line Antiretroviral Regimen for at Least Six Months Clinical failure Occurrence of new or recurrent WHO stage 3 or 4 condition ab CD4 cell failure c ·Fall of CD4 count to pre-therapy baseline (or below) or ·50% fall from the on-treatment peak value (if known) or ·Persistent CD4 levels < 100 cells/mm3 d Virological failure Plasma HIV-1 RNA level >10,000 copies/ml e a.This event must be differentiated from the immune reconstitution inflammatory syndrome (IRIS) b. Pulmonary TB and some types of extra pulmonary TB (simple glandular TB or pleural effusion) should not be automatically considered treatment failure unless there are other clinical signs of HIV disease progression. (See section 11) c.Without concomitant infection to cause transient CD4 cell decrease d.Certain experts consider that patients with persistent CD4 cell count <50/mm3 after 12 months on ART may be more appropriate e.The optimal viral load value at which ART should be switched has not been defined. However, the value of more than 10,000 copies/ml have been associated with subsequent clinical progression and appreciable CD4 cell count decline
WHO Stage 1 WHO Stage 2 WHO Stage 3 WHO Stage 4 CD4 failureb (Viral load testing not available) Do not switch regimen. Follow patient for development of clinical signs or symptoms. Repeat CD4 in 3 months. Do not switch regimen. Follow patient for evidence of further clinical progression. Repeat CD4 in 3 months. Consider switcha to second- line regimen. Recommend switch a to second- line regimen. CD4 failure b and viral load failurec Consider switch to second-line regimen. Switchto second-line regimen. Switchto second-line regimen. Switchto second-line regimen. aSwitching from first- to second-line regimen for treatment failure should not be done until the first regimen has been given sufficient time to succeed. This should be a minimum 6 month period. With only one second-line regimen available in most circumstances, premature switching should be avoided. b CD4 failure is defined as a fall to (or below) the pre-treatment baseline or a 50% drop from the on-treatment peak level or persistent levels < 100 cells/mm3 c Virological failure is provisionally defined as a plasma HIV-1 RNA level >10,000 copies/ml after a minimum of 6 months on therapy.
Standard 2nd line option if NRTI/NNRTI approach were used in 1st line TDF or ddI PI/r* EFV or NVP NRTI sparing option if simplified triple NRTI approach were used in 1st line ABC or AZT± 3TC#
First Line Regimen Second Line Regimen RTI Component PI Component b Standard Strategy AZT or d4T + 3TC a + NVP or EFV ddI + ABC or TDF + ABC or TDF + AZT ± 3TC c PI/r d TDF + 3TC a + NVP or EFV ddI + ABC or ddI + AZT ± 3TC c ABC + 3TC a + NVP or EFV ddI + AZT ± 3TC c or TDF + AZT ± 3TC c Alternative Strategy AZT or d4T + 3TC a + TDF or ABC EFV or NVP ± ddI or EFV or NVP ± 3TC c
CD4 Cell Count ART recommendations Timing of ART in relation the start of TB treatment Initiating first line ART in relationship to starting anti-TB therapy CD4 200 mm3 Recommend ART a Between 2-8 weeks b CD4 between 200-350/mm3 Recommend ART After 8 weeks CD4 350 mm3 Delay ART c Re-evaluate patient at 8 weeks and at the end of TB treatment CD4 not available Recommend ART d Between 2-8 weeks a EFV containing regimen is the preferred first line regimen. Alternative first line treatment regimens to the EFV include NVP, TDF or ABC containing regimens. For NVP containing regimens ALT should be checked at 4, 8 and 12 weeks and symptom directed thereafter b Start ART as soon as TB treatment is tolerated (between 2and 8 weeks) c If other non-TB Stage 3 or 4 events are present, start ART earlier. d For some TB diagnoses (i.e. Lymph node TB, uncomplicated pleural effusion) consider delaying ART