Download
1 / 61
610 likes | 626 Views
Nutrition for Patients with Disorders of the Lower GI Tract and Accessory Organs Chapter 18. Nutrition for Patients with Disorders of the Lower GI Tract. Ninety percent to 95% of nutrient absorption occurs in the first half of the small intestine.

E N D
Nutrition for Patients with Disorders of the Lower GI Tract and Accessory OrgansChapter 18
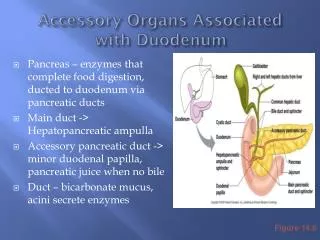
Nutrition for Patients with Disorders of the Lower GI Tract • Ninety percent to 95% of nutrient absorption occurs in the first half of the small intestine. • Large intestine absorbs water and electrolytes and promotes the elimination of solid wastes. • Accessory organs—liver, gallbladder, and pancreas—play vital roles in nutrient digestion. • Nutrition therapy is used to • Improve or control symptoms • Replenish losses • Promote healing
Altered Bowel Elimination • Constipation • Difficult or infrequent passage of stools that are hard and dry • Can occur secondary to irregular bowel habits, psychogenic factors, lack of activity, chronic laxative use, inadequate intake of fluid and fibre, metabolic and endocrine disorders, and bowel abnormalities (e.g., tumors, hernias, strictures) • Certain medications cause constipation.
Altered Bowel Elimination—(cont.) • Constipation—(cont.) • Nutrition therapy • Constipation is treated by treating the underlying cause. • Increasing fibre and fluid intake effectively relieves and prevents constipation. • High-fibre diet
Altered Bowel Elimination—(cont.) • Constipation—(cont.) • Nutrition therapy—(cont.) • Adequate intake set for fibre is 25 g/day for women and 38 g/day for men. • Common practice is to recommend fibre intake be gradually increased. • fibre intake should be spread throughout the day. • Lifestyle changes to promote bowel regularity include drinking more fluid and increasing exercise.
Altered Bowel Elimination—(cont.) • Diarrhea • Characterized by more than three bowel movements a day of large amounts of liquid or semiliquid stool • Potential for dehydration, hyponatremia, hypokalemia, acid–base imbalance (loss of bicarbonate in stool), and hence metabolic acidosis • Chronic diarrhea can lead to malnutrition related to impaired digestion, absorption, and intake.
Altered Bowel Elimination—(cont.) • Diarrhea—(cont.) • Osmotic diarrhea occurs when there is an increase in particles in the intestine, which draws water in to dilute the high concentration. • Causes include maldigestion of nutrients (e.g., lactose intolerance), excessive intake of sorbitol or fructose, dumping syndrome, tube feedings, and some laxatives. • Cured by treating the underlying cause
Altered Bowel Elimination—(cont.) • Diarrhea—(cont.) • Secretory diarrhea • Related to an excessive secretion of fluid and electrolytes into the intestines • Caused by infections, some medications, some GI disorders, and an excessive amount of bile acids or unabsorbed fatty acids in the colon • Treatment • Antibiotics if cause is infection • Symptoms may be treated with medications that decrease GI motility or thicken the consistency of stools.
Altered Bowel Elimination—(cont.) • Diarrhea—(cont.) • Nutrition therapy • Primary nutritional concern with diarrhea is maintaining or restoring fluid and electrolyte balance. • Mild diarrhea lasting 24 to 48 hours • Usually requires no nutrition intervention other than encouraging a liberal fluid intake to replace losses • High-potassium foods are encouraged (to replace lost potassium); clear liquids are avoided because they have high osmolality related to their high sugar content, which may promote osmotic diarrhea.
Altered Bowel Elimination—(cont.) • Diarrhea—(cont.) • Nutrition therapy—(cont.) • For more serious cases, commercial (e.g., Pedialyte, Rehydralyte) or homemade oral rehydration solutions, or IV therapy, are used to replace fluid and electrolytes. • May improve by avoiding foods that stimulate GI motility (e.g. high fibre) • A low-fibre diet that is also low in fat and lactose may help decrease bowel stimulation.
Malabsorption Disorders • Occurs secondary to nutrient maldigestion or from alterations to the absorptive surface of the intestinal mucosa • Malabsorption related to maldigestion involves one or few nutrients. • Malabsorption that stems from an altered mucosa is more generalized, resulting in multiple nutrient deficiencies and weight loss. • Symptoms vary with the underlying disorder.
Malabsorption Disorders—(cont.) • Excretion of fat in the stool means that essential fatty acids, fat-soluble vitamins, calcium, and magnesium are also lost through the stool. • Can cause metabolic complications
Malabsorption Disorders—(cont.) • Goal of nutrition therapy for malabsorption syndromes is to: • Control steatorrhea • Promote normal bowel elimination • Restore optimal nutritional status • Promote healing, when applicable • Individualized according to symptoms and complications
Malabsorption Disorders—(cont.) • Lactose intolerance • Occurs when the level of lactase is absent or deficient • Lactose digestion is impaired. • Undigested lactose increases the osmolality of the intestinal contents. • May lead to osmotic diarrhea
Malabsorption Disorders—(cont.) • Lactose intolerance—(cont.) • Lactose is fermented in the colon. • Produces bloating, cramping, and flatulence
Malabsorption Disorders—(cont.) • Lactose intolerance—(cont.) • Primary lactose intolerance occurs in “well” people who simply do not secrete adequate lactase. • Least common in people of northern European descent • May be asymptomatic when doses less than 4 to 12 g of lactose are consumed (e.g., ⅓ to 1 cup of milk) or when lactose is consumed as part of a meal • Chocolate milk is usually better tolerated than plain milk.
Malabsorption Disorders—(cont.) • Lactose intolerance—(cont.) • Primary lactose intolerance • Know individual limits • Lactose-reduced milk and lactase enzyme tablets (taken orally) (e.g. Lactaid) or liquid drops with lactase (e.g. Lacteeze, Lactaid) can be added to liquid foods containing lactose (e.g. milk).
Malabsorption Disorders—(cont.) • Lactose intolerance—(cont.) • Lactose intolerance secondary to gastrointestinal disorders that alter the integrity and function of intestinal villi cells, where lactase is secreted • Loss of lactase may also develop secondary to malnutrition because the rapidly growing intestinal cells that produce lactase are reduced in number and function. • Tends to be more severe than primary lactose intolerance
Malabsorption Disorders (cont’d) • Lactose intolerance—(cont.) • Nutrition therapy • Nutrition therapy for lactose intolerance is to reduce lactose to the maximum amount tolerated by the individual. • A lactose-free diet is not realistic.
Malabsorption Disorders—(cont.) • Inflammatory bowel disease (IBD) • Primarily refers to two chronic inflammatory GI diseases • Crohn disease • Ulcerative colitis • IBD is believed to be caused by an abnormal immune response to a complex interaction between environmental and genetic factors.
Malabsorption Disorders—(cont.) • Inflammatory bowel disease (IBD)—(cont.) • Characterized by periods of exacerbation and remission • Share symptoms and treatment
Malabsorption Disorders—(cont.) • Inflammatory bowel disease (IBD)—(cont.) • Nutrition therapy • Depends on the presence and severity of symptoms, the presence of complications, and the nutritional status of the patient • Diet restrictions are kept to a minimum. • Patients are often reluctant to eat. • Crohn disease is more likely to cause nutritional complications.
Malabsorption Disorders—(cont.) • Inflammatory bowel disease (IBD)—(cont.) • Nutrition therapy—(cont.) • Focus of therapy for acute exacerbation of IBD is to correct deficiencies by providing nutrients in a form the patient can tolerate. • For patients consuming an oral diet, low fibre is recommended to minimize bowel stimulation. • Protein and calorie needs are elevated to facilitate healing. • Diet modifications are made according to symptoms.
Malabsorption Disorders—(cont.) • Coeliac disease • A genetic autoimmune disorder characterized by chronic inflammation of the proximal small intestine mucosa • Related to a permanent intolerance to certain proteins found in wheat, barley, and rye • Malabsorption of carbohydrates, protein, fat, vitamins, and minerals may occur, resulting in diarrhea, flatulence, weight loss, and vitamin and mineral deficiencies.
Malabsorption Disorders—(cont.) • Coeliac disease—(cont.) • Symptoms and their severity vary depending on the patient’s age and the duration and extent of the disease. • Classic symptoms in children are diarrhea, abdominal distention, and failure to thrive. • Adults present with diarrhea, constipation, weight loss, weakness, flatus, abdominal pain, and vomiting.
Malabsorption Disorders—(cont.) • Coeliac disease—(cont.) • Atypical presentations • In 15% to 25% of people with coeliac disease, dermatitis herpetiformis is the presenting symptom. • Symptoms of dermatitis herpetiformis respond to a gluten-free diet.
Malabsorption Disorders—(cont.) • Coeliac disease—(cont.) • People who have a first-degree relative with coeliac disease, people with Down syndrome, and those with an autoimmune disease are at risk for coeliac disease. • Untreated coeliac disease is associated with an increased incidence of small bowel cancers and enteropathy-associated T-cell lymphoma.
Malabsorption Disorders—(cont.) • Coeliac disease—(cont.) • Nutrition therapy • Only scientifically proven treatment for coeliac disease is to completely and permanently eliminate gluten from the diet (example of gluten containing foods-wheat, rye, barley etc). • Lactose intolerance secondary to coeliac disease may be temporary or permanent.
Malabsorption Disorders—(cont.) • Coeliac disease—(cont.) • Nutrition therapy—(cont.) • A gluten-free diet requires a major lifestyle change. • Expensive • Short bowel syndrome (SBS) • Occurs when the bowel is surgically shortened to the extent that the remaining bowel is unable to absorb adequate levels of nutrients to meet the individual’s needs
Malabsorption Disorders—(cont.) • Short bowel syndrome (SBS)—(cont.) • Most common reasons for extensive intestinal resections that result in SBS • Crohn disease • Traumatic abdominal injuries • Malignant tumors • Mesenteric infarction
Malabsorption Disorders—(cont.) • Short bowel syndrome (SBS)—(cont.) • Nutrition complications experienced by people with short bowel syndrome depend on the amount and location of resected and remaining bowel. • Patients who have 150 cm or more of remaining small bowel without a colon, or 60 to 90 cm of small bowel with a colon, initially require PN and may progress to an oral diet over a 1- to 2-year period.
Malabsorption Disorders—(cont.) • Short bowel syndrome (SBS)—(cont.) • Factors that influence adaptation • Length of remaining jejunum and/or ileum and whether the colon is present • Patient’s age • Whether the ileocecal value remains • Health of the remaining bowel • Health of the stomach, liver, and pancreas
Malabsorption Disorders—(cont.) • Short bowel syndrome (SBS)—(cont.) • Nutrition therapy • In the early months after bowel surgery, PN is the major source of nutrition and hydration. • Consuming intact nutrients promotes bowel adaptation because they stimulate blood flow to the intestine and the secretion of pancreatic enzymes and bile acids.
Malabsorption Disorders—(cont.) • Short bowel syndrome (SBS)—(cont.) • Nutrition therapy—(cont.) • Six to eight small meals per day • If the patient’s colon is intact, fat intake is restricted to avoid steatorrhea and increased fluid losses.
Conditions of the Large Intestine • Irritable bowel syndrome (IBS) • Many factors involved in its etiology (genetics, stress to name but two) • Symptoms include lower abdominal pain, constipation, diarrhea, alternating periods of constipation and diarrhea, bloating, and mucus in the stools. • Can significantly impair quality of life
Conditions of the Large Intestine—(cont.) • Irritable bowel syndrome (IBS)—(cont.) • Nutrition therapy • Inconclusive evidence for any of the current treatments used for IBS • Pharmacologic treatment options • Meet with limited success • Complementary therapies (peppermint oil and probiotics (in yoghurt, kefir for example) MAY help • Elimination diet –trying to eliminate potential food intolerances or allergies (elimination of free fructose works for some)
Conditions of the Large Intestine—(cont.) • Irritable bowel syndrome (IBS)—(cont.) • Nutrition therapy—(cont.) • Good evidence exists for the use of 5 g of guar gum daily. • Guar gum is a soluble, nongelling fibre.
Conditions of the Large Intestine—(cont.) • Diverticular disease • Diverticula are caused by increased pressure within the intestinal lumen. • Usually asymptomatic • Diverticulitis occurs when diverticula become inflamed.
Conditions of the Large Intestine—(cont.) • Diverticular disease—(cont.) • Symptoms of diverticulitis • Cramping • Alternating periods of diarrhea and constipation • Flatus • Abdominal distention • Low-grade fever
Conditions of the Large Intestine—(cont.) • Diverticular disease—(cont.) • Potential complications • Occult blood loss and acute rectal bleeding leading to iron deficiency anemia • Abscesses and bowel perforation leading to peritonitis • Fistula formation causing bowel obstruction • Bacterial overgrowth (in small bowel diverticula) that leads to malabsorption of fat and vitamin B12
Conditions of the Large Intestine—(cont.) • Diverticular disease—(cont.) • Nutrition therapy • Despite a lack of proven efficacy, a high-fibre intake may prevent and improve symptoms of diverticulosis and prevent diverticulitis. • Once diverticula occur a high fibre diet cannot make them disappear • Avoid nuts, seeds, and popcorn to avoid them being trapped in diverticula-proposed but no scientific evidence.
Conditions of the Large Intestine—(cont.) • Diverticular disease—(cont.) • Nutrition therapy—(cont.) • During an acute phase of diverticulitis • Patients are NPO until bleeding and diarrhea subside. • Oral intake resumes with clear liquids and progresses to a low-fibre diet until inflammation and bleeding are no longer a risk. • Thereafter a high-fibre diet is recommended unless symptoms of diverticulitis recur.
Conditions of the Large Intestine—(cont.) • Ileostomies and colostomies • Performed after part or all the colon, anus, and rectum are removed • Potential nutritional problems • The smaller the length of remaining colon, the greater the potential for nutritional problems-reduced absorption of fluid, potassium and sodium. • Ileostomies cause a decrease in fat, bile acid, and vitamin B12 absorption.
Conditions of the Large Intestine—(cont.) • Ileostomies and colostomies—(cont.) • Effluent from an ileostomy is liquidy, and fluid and electrolyte losses are considerable. • Effluent through a colostomy varies from liquid to formed stools. • Nutrition therapy • Goals of nutrition therapy for ileostomies and colostomies are to minimize symptoms and replenish losses.
Conditions of the Large Intestine—(cont.) • Ileostomies and colostomies—(cont.) • Nutrition therapy—(cont.) • Initially, only clear liquids that are low in simple sugars to reduce osmotic diarrhea • Advanced slowly based on individual tolerance • Fear of eating is common. • A near-regular diet resumes 6 to 8 weeks after surgery. • Obtaining adequate fluid and electrolytes is a major concern.
Disorders of the Accessory GI Organs • Liver disease • After absorption, almost all nutrients are transported to the liver. • Vital for detoxifying drugs, alcohol, ammonia, and other poisonous substances • Liver damage can have profound and devastating effects on the metabolism of almost all nutrients.
Disorders of the Accessory GI Organs—(cont.) • Liver disease—(cont.) • Early symptoms of hepatitis • Anorexia, nausea and vomiting, fever, fatigue, headache, and weight loss • Later • Dark-colored urine, jaundice, liver tenderness, and, possibly, liver enlargement may develop. • Cell damage reversible with proper rest and nutrition
Disorders of the Accessory GI Organs—(cont.) • Liver disease—(cont.) • Acute hepatitis advances to chronic hepatitis, which may lead to cirrhosis, liver cancer, and liver failure. • Glucose intolerance is common.