Download
1 / 25
270 likes | 563 Views
Blood Gases, pH and Buffer system. Part 2. Oxygen. Role of O 2 in metabolism is crucial to all life Synthesis of ATP from ADP Evaluation of patient’s oxygen status is possible using PO 2 measured along with PCO 2 and pH in blood gas analysis

E N D
Oxygen • Role of O2 in metabolism is crucial to all life • Synthesis of ATP from ADP • Evaluation of patient’s oxygen status is possible using PO2 measured along with PCO2 and pH in blood gas analysis • In patients with respiratory disorders, a disturbance of the partial pressure of oxygen (PO2) may be of greater clinical significance than either an abnormal PCO2 or abnormal [H+]. M. Zaharna Clin. Chem. 2009
Tissue oxygenation • For adequate tissue oxygenation the following conditions are necessary: • Available atmospheric O2 • Adequate ventilation • Gas exchange is sufficient (lung & arterial blood) • Loading of O2 onto Hemoglobin • Adequate Hemoglobin • Adequate transport and release mechanism of O2 is properly working. • Any disturbances in these conditions can result in poor tissue oxygenation M. Zaharna Clin. Chem. 2009
Oxygen Transport • Most of the O2 in arterial blood is transported to the tissues by Hb. • The amount of O2 loaded onto Hb depends on the following: • availability of O2. • concentration and types of Hb present. • presence of nonoxygen substances such as CO. • H+ (pH). • blood temperature. • pCO2 levels. • 2,3-DPG levels. • With normal diffusion of O2 to the arterial blood, more than 95% of the functional Hb (hemoglobin capable of reversibly binding O2 )will bind O2. M. Zaharna Clin. Chem. 2009
Blood Hb • Blood Hb exists in one of four conditions: • Oxyhemoglobin (O2Hb), O2 is reversibly bound to Hb. • Deoxyhemoglobin (HHb), Hb not bound to O2, but is capable of forming a bond when O2 is available. • Carboxyhemoglobin (COHb), the bond between CO and Hb is reversible, • but is > 200 times as strong as the bond between O2 and Hb. • Methemoglobin (Met-Hb), Hb unable to bind O2 because Fe is in the oxidized state. • Fe+3 can be reduced by the enzyme metHb-reductase which is found in RBCs. M. Zaharna Clin. Chem. 2009
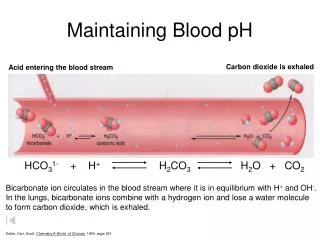
Hemoglobin-Oxygen dissociation • O2 dissociates from Adult hemoglobin (Hb-A) readily. • Hb holds on the O2 until O2 tension is reduced to 60 mmHg- then O2 released rapidly. • In tissue, exposure to elevated CO2 and H+ results in enhanced O2 release. • This release of oxygen from hemoglobin accelerates the uptake of CO2 and H+ by hemoglobin (acid-base buffering). • In the lungs, the microenvironment promotes uptake of O2 and release of CO2. M. Zaharna Clin. Chem. 2009
Hemoglobin-Oxygen dissociation In addition to adequate ventilation and gas exchange with the pulmonary circulation, O2 must be released at the tissues. Hemoglobin transports O2. The increased H+ concentration and pCO2 levels at the tissue from cellular metabolism change the molecular configuration of O2Hb, facilitating O2 release. M. Zaharna Clin. Chem. 2009
Hemoglobin-Oxygen dissociation Oxygen dissociates from adult hemoglobin (A1) in a characteristic fashion. If this dissociation is graphed with pO2 on the x-axis and percent SO2 on the y-axis, the resulting curve is slightly S shaped. Hemoglobin “holds on” to O2 until the O2 tension in the tissue is reduced to about 60 mm Hg. Below this tension, the O2 is released rapidly. The position of the oxygen dissociation curve reflects the affinity that hemoglobin has for O2 and affects the rate of this dissociation. M. Zaharna Clin. Chem. 2009
26 mmHg 40 mmHg M. Zaharna Clin. Chem. 2009
Factors effecting the affinity of Hb for O2 • Shift to the right "decreased affinity", Hb releases O2 more easily due to the following factors: • increase in H+ "low pH" • increased PCO2 • increased temperature • increased 2,3-DPG concentration. • Shift to left" increased affinity of Hb for O2 and decreased release of O2" due to the following factors: • Decrease in H+ "elevated pH" • Decrease in PCO2 • Decrease in temperature • Decrease in 2,3-DPG concentration. M. Zaharna Clin. Chem. 2009
Patient’s Oxygen Status • Four parameters commonly used to assess a patient’s oxygen status: • Oxygen saturation • It represents the ratio of O2 that is bound to Hb, compared with the total amount of Hb capable of binding O2 • Fractional (or percent) oxyhemoglobin (FO2Hb) • The ratio of the concentration of oxyHb to the concentration of total Hb M. Zaharna Clin. Chem. 2009
Patient’s Oxygen Status • where the cdysHb (dyshemoglobins)represents hemoglobin derivatives, such as COHb • Trends in oxygen saturation • By oximeter, differentiate between oxyhemoglobin and deoxyhemoglobin • Amount of O2 dissolved in plasma • PO2 → 90 – 95 mm Hg • For an adult blood volume of 5 L, only 13.5 mL of O2 will be available from pO2 in plasma, compared with more than 1,000 mL of O2 carried as O2Hb M. Zaharna Clin. Chem. 2009
Collection and Handling of Specimen The specimen for blood gases and pH should be arterial blood collected in heparinized plastic containers including syringes All air bubbles should be removed before mixing the specimen, The needle replaced or the ends of the capillary tube fitted with a tight-fitting cover M. Zaharna Clin. Chem. 2009
Collection and Handling of Specimen • The specimen must be placed in ice water until analysis, unless it is analyzed immediately at the patient’s bedside. • Temperatures warmer than 4oC allow: • cell glycolysis to continue in the whole blood specimen, • resulting in falsely decreased pH • and partial pressure of oxygen (PO2) • and falsely increased partial pressure of carbon dioxide (PCO2). M. Zaharna Clin. Chem. 2009
Pulse Oximetry Noninvasive measurements for following “trends” in oxygenation are attained with pulse oximetry (SpO2). These devices pass light of two or more wavelengths through the tissue in the capillary bed of the toe, finger, or ear. Until recently, pulse oximetry technology could not measure COHB and MetHb. For those pulse oximeters that calculate oxyHb saturation based only on oxyHb and deoxyHb, oxyHb saturation will be overestimated when one or more dyshemoglobins are present. In addition, the accuracy of pulse oximetry can be compromised by many factors, including poor perfusion and severe anemia. M. Zaharna Clin. Chem. 2009
Measurements Spectrophotometric ( co-oximeter) • Co-oximeter designed to determine various Hb species directly • Each species has a characteristic absorbance curve • Instruments should have 4 W.L. for: • HHb, O2Hb, COHb and MetHb M. Zaharna Clin. Chem. 2009
Absorption Spectra of Hemoglobins M. Zaharna Clin. Chem. 2009
Blood Gas Analyzer • Arterial blood anticoagulated with heparin is used for gas analysis • Hydrogen ion concentration [H+] in arterial blood is measured. • The arteriovenous difference for [H+] is small (<2 nmol/L), M. Zaharna Clin. Chem. 2009
Blood Gas Analyzer • but the difference is significant for PCO2 approximately 6 mmHg higher in venous blood. • and PO2, 50 mmHg lower in venous blood. • Use electrode method for sensing and measuring: • PO2 • PCO2 • pH M. Zaharna Clin. Chem. 2009
Arterial blood gas reference range at 37oC M. Zaharna Clin. Chem. 2009
Case Study As part of a class experiment in physiology, a medical student volunteered to have a sample of arterial blood taken. The demonstrator took some time to explain the procedure to the class, during which time the student became increasingly anxious. As the blood was being drawn she complained of tingling in her fingers and toes. M. Zaharna Clin. Chem. 2009
Comment The student is alkalotic with a low PCO2, thus the disturbance is respiratory in origin. The extent of the decrease in [H+] indicates that there is neither compensation nor an additional acid-base disturbance. The low PCO2 is a result of anxiety-induced hyperventilation and no compensation would be expected to have occurred in this short time. The symptoms are a result of a decrease in the concentration of ionized calcium, an effect of alkalosis. M. Zaharna Clin. Chem. 2009
Case Study A young woman was admitted to hospital 8 h after she had taken an overdose of aspirin. M. Zaharna Clin. Chem. 2009
Comment There is an acute respiratory alkalosis with a coexistent non-respiratory acidosis. This combination is characteristic of salicylate poisoning, where initial respiratory stimulation causes a respiratory alkalosis but later the metabolic effects of salicylate tend to predominate, producing an acidosis. This case history illustrates the importance of considering the clinical setting when analyzing acid-base data. Calculation of the anion gap might have been helpful here. It would have been increased by the presence of organic anions, indicating a coexisting non-respiratory acidosis, but is normal in respiratory alkalosis. M. Zaharna Clin. Chem. 2009