Download
1 / 1
10 likes | 164 Views
EXTRAPERITONEAL RADICAL PROSTATECTOMY AND PREVIOUS HISTORY OF HERNIA REPAIR: EVALUATION OF RESULTS SELCUK KESKIN, GUILLAUME GUICHARD, ÁNDRAS HOZNEK , ALEXANDRE DE LA TAILLE, RENE YIOU,DIMITRI VORDOS, CLEMENT-CLAUDE ABBOU and LAURENT SALOMON

E N D
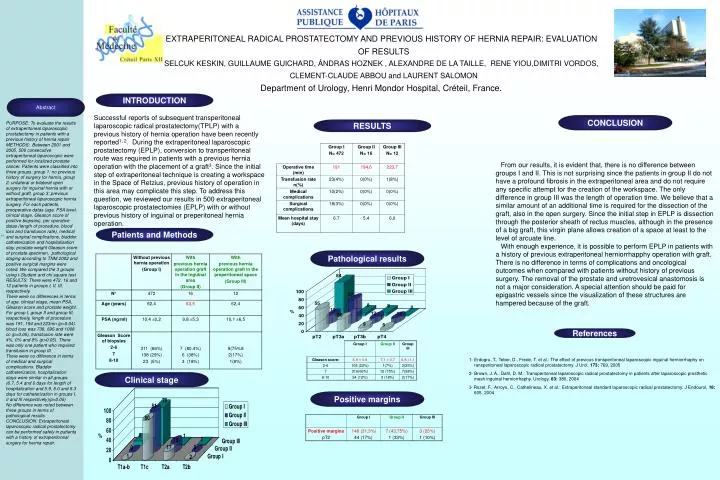
EXTRAPERITONEAL RADICAL PROSTATECTOMY AND PREVIOUS HISTORY OF HERNIA REPAIR: EVALUATION OF RESULTS SELCUK KESKIN, GUILLAUME GUICHARD, ÁNDRAS HOZNEK , ALEXANDRE DE LA TAILLE, RENE YIOU,DIMITRI VORDOS, CLEMENT-CLAUDE ABBOU and LAURENT SALOMON Department of Urology, Henri Mondor Hospital, Créteil, France. INTRODUCTION Abstract Successful reports of subsequent transperitoneal laparoscopic radical prostatectomy(TPLP) with a previous history of hernia operation have been recently reported1, 2. During the extraperitoneal laparoscopic prostatectomy (EPLP), conversion to transperitoneal route was required in patients with a previous hernia operation with the placement of a graft3. Since the initial step of extraperitoneal technique is creating a workspace in the Space of Retzius, previous history of operation in this area may complicate this step. To address this question, we reviewed our results in 500 extraperitoneal laparoscopic prostatectomies (EPLP) with or without previous history of inguinal or preperitoneal hernia operation. CONCLUSION PURPOSE: To evaluate the results of extraperitoneal laparoscopic prostatectomy in patients with a previous history of hernia repair METHODS: Between 2001 and 2005, 500 consecutive extraperitoneal laparoscopic were performed for localized prostate cancer. Patients were classified into three groups: group 1: no previous history of surgery for hernia, group 2: unilateral or bilateral open surgery for inguinal hernia with or without graft, group 3: previous extraperitoneal laparoscopic hernia surgery. For each patients, preoperative datas (age, PSA level, clinical stage, Gleason score of positive biopsies), per operative datas (length of procedure, blood loss and transfusion rate), medical and surgical complications, bladder catheterization and hospitalisation stay, prostate weight Gleason score of prostate specimen, pathological staging according to TNM 2002 and positive surgical margins were noted. We compared the 3 groups using t-Student and chi square test RESULTS: There were 472, 16 and 12 patients in groups I, II, III, respectively. There were no differences in terms of age, clinical stage, mean PSA, Gleason score and prostate weight. For group I, group II and group III, respectively, length of procedure was 191, 194 and 223mn (p=0.04). blood loss was 738, 696 and 1008 cc (p>0,05), transfusion rate were 4%, 0% and 8% (p>0.05). There was only one patient who required transfusion in group III. There were no difference in terms of medical and surgical complications. Bladder catheterization, hospitalization stays were similar in all groups. (6.7, 5.4 and 6 days for length of hospitalization and 5.9, 6.0 and 5.3 days for catheterization in groups I, II and III respectively)(p>0.05) No difference was noted between three groups in terms of pathological results. CONCLUSION: Extraperitoneal laparoscopic radical prostatectomy can be performed safely in patients with a history of extraperitoneal surgery for hernia repair. RESULTS From our results, it is evident that, there is no difference between groups I and II. This is not surprising since the patients in group II do not have a profound fibrosis in the extraperitoneal area and do not require any specific attempt for the creation of the workspace. The only difference in group III was the length of operation time. We believe that a similar amount of an additional time is required for the dissection of the graft, also in the open surgery. Since the initial step in EPLP is dissection through the posterior sheath of rectus muscles, although in the presence of a big graft, this virgin plane allows creation of a space at least to the level of arcuate line. With enough experience, it is possible to perform EPLP in patients with a history of previous extraperitoneal herniorrhapphy operation with graft. There is no difference in terms of complications and oncological outcomes when compared with patients without history of previous surgery. The removal of the prostate and uretrovesical anastomosis is not a major consideration. A special attention should be paid for epigastric vessels since the visualization of these structures are hampered because of the graft. Patients and Methods 21. Pathological results References 1- Erdogru, T., Teber, D., Frede, T. et al.: The effect of previous transperitoneal laparoscopic inguinal herniorrhaphy on ransperitoneal laparoscopic radical prostatectomy. J Urol, 173: 769, 2005 2- Brown, J. A., Dahl, D. M.: Transperitoneal laparoscopic radical prostatectomy in patients after laparoscopic prosthetic mesh inguinal herniorrhaphy. Urology, 63: 380, 2004 3- Rozet, F., Arroyo, C., Cathelineau, X. et al.: Extraperitoneal standard laparoscopic radical prostatectomy. J Endourol, 18: 605, 2004 Clinical stage Positive margins