Download
1 / 31
310 likes | 643 Views
Hypoparathyroidism: Evaluation and Management-Dr Selim

E N D
Hypoparathyroidism Evaluation & Management Dr Shahjada Selim Associate Professor Department of Endocrinology, BSMMU, Bangladesh https://shahjadaselim.com
Outlines • Understand the calcium and related hormones physiology • Understand the hypoparathyroidism • Understand hyperparathyroidism
Normal physiology • Parathyroid hormone (PTH) plays a key role in the regulation of calcium and phosphate homeostasis and vitamin D metabolism • The PTH acts directly on the bones and kidneys and indirectly on the intestine through its effect on the synthesis of 1,25 (OH)2D3. PTH increase the kidney production of active vitamin D • Its production is regulated by the concentration of serum ionized calcium. Lowering of the serum calcium levels will induce an increased rate of parathyroid hormone secretion • Calcitonin is released by the “C” cells (Para-follicular cells in the thyroid gland) in response to small increases in plasma ionic calcium
Normal physiology • Calcitonin acts on the kidney and bones to restore the level of calcium to just below a normal set point which in turn inhibits secretion of the hormone • Calcitonin is therefore the physiological antagonist of PTH. The two hormones act in concert to maintain normal concentration of calcium ion in the extracellular fluid • 1,25 (OH)2D3: Calcitriol also called 1,25-dihydroxycholecalciferol or 1,25- dihydroxyvitamin D3
Nutshell • Calcium metabolism gets controlled in the body by 3 players AND 3 hormones (bone, Kidney, intestine) VS (PTH, Vitamin D, Calcitonin): • PTH: - ↑ Bone resorption. - ↑ Calcium reabsorption from kidney - ↓ Phosphate reabsorption • Vitamin D: - ↑ Calcium absorption from intestine - ↑ Calcium reabsorption from kidney - ↑ Phosphate reabsorption • Calcitonin: - ↓ Bone resorption. - ↑ Calcium reabsorption from kidney - ↑ Phosphate reabsorption
Ø Parathyroid hormone regulates calcium homeostasis by a tightly controlled system. Ø PTH plays an important role in mobilizing calcium from the skeleton where calcium is primarily stored and increasing calcium absorption from the intestine by increasing synthesis of calcitriol (1,25-dihydroxyvitamin D) from the kidney. Ø Increased conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D occurs in the proximal renal tubule. Ø PTH also increases calcium reabsorption from the thick ascending limb of nephrons and facilitates the excretion of phosphorus through the kidneys.
Ø Calcium is sensed by the CaSR, a 7-transmembrane G protein-coupled receptor found on the parathyroid glands, which stimulates PTH release in response to low serum calcium, and suppresses PTH release in response to high serum calcium. Ø The CaSR is also expressed in several other tissues including renal tubular cells, where it regulates calcium reabsorption, as well as bone and intestinal cells. Ø In hypercalcemia, the filtered calcium load overcomes the renal tubular ability to reabsorb calcium resulting in decrease in calcium and sodium transport in the loop of Henle with an associated decrease in urinary concentrating ability to reduce calcium absorption through the kidneys.
Ø When the production of PTH is reduced or absent, low PTH is inadequate to maintain normocalcemia and normophosphatemia, thus the biochemical findings of the disease, such as hypocalcemia, hyperphosphatemia, and low PTH ensue. Ø The most common cause of hypoparathyroidism is inadvertent damage to the parathyroid glands during thyroid surgery (1-3). Other causes of hypocalcemia that need to be ruled out include magnesium deficiency and vitamin D deficiency. Ø Magnesium is needed for the secretion of PTH by the parathyroid glands and its depletion or excess may cause hypoparathyroidism and subsequent hypocalcemia. Ø This is thought to be due to the lack or excess magnesium playing a role in defective cyclic AMP generation in the parathyroid glands interfering with PTH synthesis and secretion (4). 1.Stack BC, Jr, Bimston DN, Bodenner DL, Brett EM, Dralle H, Orloff LA, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Disease state clinical review: postoperative hypoparathyroidism – definitions and management. Endocr Pract (2015) 21(6):674–85. 10.4158/ep14462.dsc 2,Mannstadt M, Clarke BL, Vokes T, Brandi ML, Ranganath L, Fraser WD, et al. Efficacy and safety of recombinant human parathyroid hormone (1-84) in hypoparathyroidism (REPLACE): a double-blind, placebo-controlled, randomised, phase 3 study. Lancet Diabetes Endocrinol (2013) 1(4):275–83. 10.1016/S2213-8587(13)70106-2 3. Shoback DM, Bilezikian JP, Costa AG, Dempster D, Dralle H, Khan AA, et al. Presentation of hypoparathyroidism: etiologies and clinical features. J Clin Endocrinol Metab (2016) 101(6):2300–12. 10.1210/jc.2015-3909 4. Rude RK, Oldham SB, Singer FR. Functional hypoparathyroidism and parathyroid hormone end-organ resistance in human magnesium deficiency. Clin Endocrinol (Oxf) (1976) 5(3):209–24. 10.1111/j.1365-2265.1976.tb01947.x
There are three types of parathyroid disease: •Hypoparathyroidism. •Hyperparathyroidism •Parathyroid cancer and
Hypoparathyroidism Hypoparathyroidism is a relatively rare endocrine disorder in which parathyroid hormone (PTH) which manifests itself biochemically by hypocalcaemia,, hyperphosphatemia, diminished or absent circulating iPTH (immunoreactive parathyroid hormone) and clinically the symptoms of neuromuscular hyperactivity.
Surgical hypoparathyroidism Causes: • Surgical hypoparathyroidism, the commonest a. After anterior neck exploration for thyroidectomy, abnormal parathyroid gland removal, excision of a neck lesion. b. It could be due to the removal of the parathyroid glands or due to interruption of blood supply to the glands. c. Radical surgery for head and neck malignancies. (Surgeons always be aware of 2 things- parathyroid glands and recurrent laryngeal nerves)
Idiopathic hypoparathyroidism An early age (genetic origin) with autosomal recessive mode of transmission a) Multiple endocrine deficiency, Autoimmune-candidiasis (MEDAC) syndrome. b) Juvenile familial endocrinopathy, c) Hypoparathyroidism , Addison's disease, mucocutaneous candidiasis(HAM)syndrome. • Circulating antibodies for the parathyroid glands and the adrenals are frequently present. • Other associated disease: • Pernicious anemia • Ovarian failure • Autoimmune thyroiditis • Diabetes mellitus • The late onset form occurs sporadically without circulating grandular autoantibodies
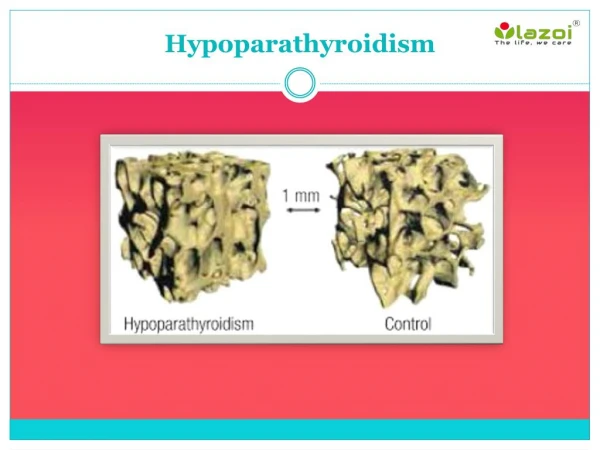
Hungry Bone Syndrome The term ‘hungry bone syndrome’ (HBS) has been coined to the profound (serum calcium <2.1 mmol/l) and prolonged (longer than 4th day post-operatively) hypocalcaemia, which follows parathyroidectomy for severe hyperparathyroidism. This is usually associated with skeletal manifestations, reflected by high preoperative indices of bone turnover, osteitis fibrosa cystica and/or ‘brown tumours’. The severe hypocalcaemia is believed to be due to the greatly increased skeletal usage of calcium, thought to occur as a result of removal of the effect of high circulating parathyroid hormone (PTH) levels on bone, with immediate arrest of bone resorption in the face of continuing and enhanced bone formation, although there is no good documentation for this.
Hungry Bone Syndrome This decrease in serum calcium levels is usually mild and maximal 2–4 days post-operatively, and independent of the size of hyperactive glands or pathological diagnosis. Persistence of hypocalcaemia for more than 4 days after parathyroidectomy may be due to intentional or accidental removal of all parathyroid glands, devascularisation or trauma to residual parathyroid glands, but is also often due to long-term suppression of residual non-pathological parathyroid glands.
Epidemiology Available data regarding the prevalence of HBS is varied and has changed, expectedly so, overtime. In the past, it was estimated to occur in approximately 13% of cases post parathyroidectomy for primary hyperparathyroidism, but more recently, in case series, reports are as low as 4%. One specific case came from a population of patients from Saudi Arabia and likely mirrors a rate closer to the current expectation in the U.S. However; other data suggest a rate as high as 87% in a cohort of patients in an Asian population. A possible theory is that this vast difference might be related to better access to care and earlier diagnosis with subsequent timely treatment of hyperparathyroidism leading to a lesser prevalence of HBS.
Epidemiology Regarding cases post parathyroidectomy for secondary hyperparathyroidism, the prevalence ranges between 20 to 70%. Data regarding prevalence in tertiary hyperparathyroidism is scarce. It is noted, in one prospective study, that the prevalence of HBS in an Indian cohort of thyrotoxic patients post thyroidectomy was approximately 39%. Instances of hypocalcemia not due to post-surgical hypoparathyroidism post thyroidectomy were also noted in a study of post-operative patients in Singapore with a rate of 53%, although this study did not explicitly clarify or was able to elucidate if these were instances of HBS. For HBS in metastatic prostatic cancer, we only have case reports.
Incidence, prevalence and risk factors for post-surgical hypocalcaemia and hypoparathyroidism
Functional hypoparathyroidism Hypomagnesemia: Magnesium is necessary for PTH to be released from the gland. Low magnesium levels also lead to increased urinary loss of calcium.
Hypocalcemia with Non-Hypothyroidism causes Renal failure Leads to hypocalcemia. The kidney converts 25 hydroxy-D to the more active 1,25 hydroxy-D. (Renal failure = Loss of vitamin D) • Other causes include vitamin D deficiency, genetic disorders, fat malabsorption, and low albumin states. • Decreased intestinal absorption of vitamin D or calcium due to primary small bowel disease, short bowel syndrome, and post-gastrectomy syndrome. Drugs that cause rickets or osteomalacia such as phenytoin, phenobarbital, cholestyramine, and laxative.
Chronic hypocalcemia other than parathyroidal hypoparathyroidism • States of tissue resistance to vitamin D • Excessive intake of inorganic phosphate compounds • Psudohypoparathyroidism • Severe hypomagnesemia • Chronic renal failure
Clinical Presentations Symptoms of hypoparathyroidism are the result of low serum calcium effect on the internal organs and correlate strongly with the acuteness of the low serum calcium as well as the absolute level. For example, a patient who has chronic hypoparathyroidism since childhood may adapt to low levels of calcium even as low as 7.0 mg/dl and remain asymptomatic. Presenting symptoms are variable. Mild symptoms include numbness and tingling of the extremities and perioral region, muscle cramps, and fatigue, and in severe cases, tetany, seizure, altered mental status, cardiac rhythm disturbances, refractory congestive heart failure, bronchospasm, and laryngospasm can be seen (1,2). In most patients, symptoms develop when the albumin-corrected serum calcium is less than 7.5–8.0 mg/dl (3) 1.Bilezikian JP, Khan A, Potts JT, Jr, Brandi ML, Clarke BL, Shoback D, et al. Hypoparathyroidism in the adult: epidemiology, diagnosis, pathophysiology, target-organ involvement, treatment, and challenges for future research. J Bone Miner Res (2011) 26(10):2317–37. 10.1002/jbmr.483 [PMC free article] [PubMed] [CrossRef] [Google Scholar] 2. Hadker N, Egan J, Sanders J, Lagast H, Clarke BL. Understanding the burden of illness associated with hypoparathyroidism reported among patients in the paradox study. Endocr Pract (2014) 20(7):671–9. 10.4158/ep13328.
Clinical Presentations • Patients with an acute drop in their serum calcium after neck surgery have more dramatic symptoms than those with chronic hypocalcemia. • Myoclonic jerks, twitching, new-onset seizures due to cerebral hypocalcemia, or worsening of seizures are neurologic manifestations of hypocalcemia. • Cardiac manifestations are prolonged QT interval and T-wave alternans, acute cardiomyopathy, and congestive heart failure due to decreased cardiac contractility related to low serum calcium and possibly PTH deficiency, as there are PTH receptors in cardiac myocytes.
• Many patients complain of cognitive dysfunction, in particular, brain fog, fatigue, and easy fatigability. Higher incidence of anxiety, depression, and overall reduced quality of life occurs in patients with hypoparathyroidism compared to normal control groups . • However, one systematic review failed to show a link between PTH and cognitive dysfunction and dementia (1), so it is assumed that these conditions are mostly due to the calcium disturbance. 1. Lourida I et al. PLoS One (2015) 10(5):e0127574. 10.1371/journal.pone.0127574
Clinical Presentations 1. Basal Ganglia Calcifications ( Fahr’s disease ) : genetically dominant inherited neurological disorder characterized by abnormal deposits of calcium in areas of the brain that control movement ( Similar to Parkinson’s disease symptoms ). 2. Prolonged QT : Severe ↓ Ca > Prolonged QT > torsades de pointes, a specific type of ventricular tachycardia ( Death ). 3. Malabsorption syndrome : Presumably secondary to decreased calcium level and may lead to steatorrhoea with long standing untreated disease. 4. Dental Manifestation : Abnormal enamel formation with delayed or absent dental eruption and defective dental root formation.
5. Rickets ,osteomalacia and Posterior lenticular cataract . 5. Rickets ,osteomalacia and Posterior lenticular cataract . • Neuromuscular irritability: When nerves are exposed to low levels of calcium they show abnormal neuronal function which may include decrease threshold of excitation, repetitive response to a single stimulus and rarely continuous activity. ○ Paresthesia ○ Latent Titany: A. Hyperactive deep tendon reflexes. B. Chvostek’s sign :Tapping the facial nerve causes contraction of facial muscles. C. Trousseau’s sign : Inflating the BP cuff to a pressure higher than the patient’s systolic BP for 3 minutes elicits carpal spasms. • Convulsions : More common in young people and it can take the form of either generalized tetany followed by prolonged tonic spasms or the typical epileptiform seizures. 6. Grand Mal seizures, Hyperventilation and Adrenergic symptoms .
Diagnosis 1. Low serum calcium. 2. High serum phosphate. 3. Serum PTH inappropriately low. 4. Low urine cAMP. (The parathyroid hormone works on Gs G protein which then leads to decreased levels of cAMP (as second messenger).
Treatment Mainstay of treatment: Combination of oral calcium with pharmacological doses of vitamin D or its potent analogues. Phosphate restriction in diet may also be useful with or without aluminum hydroxide gel to lower serum phosphate level. Emergent treatment: only give in case of symptomatic and present of neural irritability: IV calcium gluconate. Remember: Both vitamin D and calcium replacement can increase urinary calcium excretion, precipitating kidney stones. Therefore, administer with caution to avoid hypercalciuria
Imnportant Considerations • Impaired renal function is the most common complication seen in patients treated for hypoparathyroidism. It is associated with the age of the patient, duration of the disease, and level of hypercalcemia during treatment. • Absence of PTH results in inability of renal tubules to reabsorb calcium, resulting in hypercalciuria and nephrocalcinosis. • In addition, patients with underlying renal disease such as renal dysgenesis in DiGeorge syndrome are in particular at higher risk for nephrolithiasis. • Overtreatment of hypoparathyroidism with calcitriol and calcium can lead to nephrolithiasis, thus monitoring of renal calcium excretion is necessary.