Download
1 / 59
630 likes | 918 Views
Hypothyroidism: Evaluation & Management by Dr Shahjada Selim

E N D
Hypothyroidism: Evaluation & Management Dr Shahjada Selim Associate Professor, Department of Endocrinology, BSMMUVisiting Professor in Endocrinology, Texila American University, USA Website: http://shahjadaselim.com
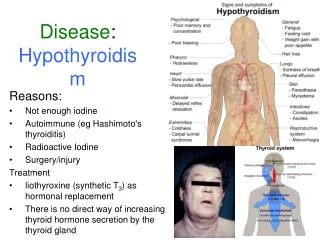
Definition Hypothyroidism means that the thyroid gland can’t make enough thyroid hormone to keep the body running normally. In hypothyroidism thyroid gland is underactive the tissues are to too little thyroid hormone. ATA 2021: https://www.thyroid.org/hypothyroidism/Accessed on 21/01/2021
Epidemiology -Hypothyroidism occurs in 3 to 6% for the adult population, but is symptomatic only in a minor of them. • Usually develops after the age of 30 • It occurs 8 to 10 times more often in women than in men
I. Congenital II. Acquired 1. Subclinical hypothyroidism 2. Clinical hypothyroidism 1. Primary (thyroid gland disturbances). 2. Secondary (due to pituitary disease). 3.Tertiary (due to hypothalamic disease). 4.Peripheral. Classification of Hypothyroidism
Congenital • Maldevelopment –hypoplasia or aplasia • Inborn deficiencies of biosynthesis or action of thyroid hormone • Atypical localization of thyroid gland • Severe iodine deficiency Primary Hypothyroidism Etiology of Hypothyroidism
iodine deficiency • autoimmune processes (Hashimoto’s thyroiditis): MAE 1 & 2 • surgical -total thyroidectomy • irradiation therapy (organs of the neck)-I131 therapy • during or after therapy with propylthyouracil, methimazole, iodides for hyperthyroidism • infiltrative diseases (tuberculosis, actynomycosis) • trauma • medications such as amiodarone, interferon alpha, thalidomide Acquired
peripheral tissue resistance to thyroid hormones • decreasing of T4 peripheral transformation into T3 (in liver or in kidneys) • production of antibodies to thyroid hormones Etiology of Peripheral Hypothyroidism
Skin & Hair • Skin is dry, thick and silk, is often cool and pale. • Nonpitting edema of the hands, feet and periorbital regions (myxedema). Pitting edema also may be present. • The faces are puffy and features are coarse. the loss of the lateral aspect of the eyebrow, sometimes termed Queen Anne's sign
Skin & Hair • Skin may be orange due to accumulation of carotene. • Hair may become course and brittle, hair growth slows and hair loss may occur. Lateral eyebrows thin out and body hair is scanty. • Hypothyroidism does not cause obesity, but modest weight gain from fluid retention and fat deposition often occurs
Nervous system Patients complain on fatigue, loss of energy, lethargy, forgetfulness, reduced memory. • Their level of physical activity decreases, and they may speak and move slowly. Mental activity declines and there is inattentiveness, decreased intellectual function, and sometimes may be depression. • Neurological symptoms include also hearing loss, parasthesias, objective neuropathy, particularly the carpal tunnel syndrome, ataxia. • Tendon reflex shows slowed or hung-up relaxation.
Cardiovascular system Complains on: dyspnea, pain in the region of the heart Objective examination: • Increased peripheral resistance • Hypertension (Diastolic) • Bradycardia • LV hypertrophy with decreased contractility, reduced cardiac output • Pericardial effusion • Congestive heart failure • The ECG may show low voltage and/or non-specific ST segment and T wave changes. • Hypercholesterolemia
Gastrointestinal System • Gastrointestinal motility is decreased loading to constipation and abdominal distension, pseudoobstruction of intestines, paralytic ileus. • Abdominal distension may be caused by ascities as well. Ascitic fluid, like other serous effusions in myxedema, has high protein content. • Achlorhydria occurs, often associated with pernicious anemia.
Reduced excretion of a water load may be associated with hyponatriemia • Renal blood flow and glomerular filtration rate are reduced, but serum creatinine is normal • May be mild proteinuria and infections of urinary tract Renal system
Respiratory system • Dyspnea of effort is common. This complaint may be caused by enlargement of the tongue and larynx, causing upper airway obstruction, or by respiratory muscle weakness, interstitial edema of the lungs, and for plural effusions which have high protein content • Hoarseness from vocal curt enlargement often occurs
Muscle and joint aches, pains and stiffness are common • Objective myopathy and joint swelling or effusions are less often present • The relaxation phase of the tendon reflexes is prolonged • Serum creatine phosphokinase and alanine aminotransferase activities are often increased, probably as much to slowed enzyme degradation as to increased release from muscle Musculoskeletal System
Blood disorders • Anemia, usually normocytic, caused by decreased red blood cell production, may occur. It is probably from decreased need of peripheral oxygen delivery rather than hematopoetic defect • Megaloblastic anemia suggests coexistent pernicious anemia • Most patients have no evidence iron, folic acid or cyancobalamin deficiency
Endocrine System • Thyroid gland: nonpalpable or enlargement. • Adrenal glands: hypofunction • Pituitary system: secretion of growth hormone is deficient because thyroid hormone is necessary for synthesis of growth hormone. Growth and development of children are retarded. Epiphyses remain open. • Gonadal glands: menorrhagia (from anovulatory cycles), secondary amenorrhea, infertility and galactorrhea; decreased fertility in men
Hypothermia is common • Hyperlipidemia with increase of serum cholesterol and triglyceride occurs because of reduced lipoprotein lipase activity Metabolic System
Clinical features • Hypothyroidism can be presented in many different ways and can mimic other disorders • Because many manifestations of hypothyroidism are non-specific, the diagnosis is particularlylikely to be overlooked in patients with otherchronic illnesses and elderly and can lead to significant morbidity and even mortality
It is an asymptomatic state in which serum T4 and free T4 are normal, but serum TSH is elevated. This designation is only applicable when thyroid function has been stable for weeks or more, the hypothalamic-pituitary-thyroid axis is normal, and there is no recent or ongoing severe illness. • It is a state in which clinical features of hypothyroidism are usually absent and euthyroidism is reached by compensatory increasing of TSH secretion and that’s why synthesis and secretion of such level of thyroid hormone that will be enough for organism. Subclinical Hypothyroidism
Rationale for Treating Subclinical Hypothyroidism • Potential benefits from treatment • Prevent progression to overt hypothyroidism • Improve serum lipid profile, which may reduce the risk of death from cardiovascular causes • Reduce symptoms, including psychiatric and cognitive abnormalities • Better fertility outcome • Improves menstrual irregularities Cooper DS. N Engl J Med. 2001;345:260-264.
Recommendations Organizations Regarding Screening ofAsymptomatic Adults for Thyroid Dysfunction
The goal of hypothyroidism therapy is to replace thyroxine to mimic normal, physiologic levels and alleviate signs, symptoms, and biochemical abnormalities Hypothyroidism Treatment Goal Euthyroidism Braverman LE, et al. Werner & Ingbar’s The Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.
Levothyroxine sodium is the treatment of choice for the routine management of hypothyroidism • Adults: about 1.7 g/kg of body weight/d • Children up to 4.0 g/kg of body weight/d • Elderly <1.0 g/kg of body weight/d • Clinical and biochemical evaluations at 6- to 8-week intervals until the serum TSH concentration is normalized • Given the narrow and precise treatment range for levothyroxine therapy, it is preferable to maintain the patient on the same brand throughout treatment Hypothyroidism Treatment Singer PA, et al. JAMA. 1995;273:808-812. Endocr Pract. 2002;8:457-469.
Initial Levothyroxine Dose 6-8 Weeks TSH >3.0 IU/mL TSH <0.5 IU/mL Repeat TSH Test TSH 0.5- 2.0 IU/mL Symptoms Resolved Primary Hypothyroidism Treatment Algorithm Increase Levothyroxine Dose by 12.5 to 25 g/d Decrease Levothyroxine Dose by 12.5 to 25 g/d Continue Dose Measure TSH at 6 Months, Then Annually or When Symptomatic Singer PA, et al. JAMA. 1995;273:808-812. Demers LM, Spencer CA, eds. The National Academy of Clinical Biochemistry Web site. Available at: http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1, 2003.
Clinical and laboratory monitoring enable • Evaluation of the clinical response • Assessment of patient compliance • Assessment of drug interactions, if applicable • Adjustment of dosage, as needed • Clinical and laboratory evaluations should be performed • At 6- to 8-week intervals while titrating • Every 6 – 12 months once a euthyroid state is established Therapy Monitoring Singer PA, et al. JAMA. 1995;273:808-812. Demers LM, Spencer CA, eds. Demers LM, Spencer CA, eds. The National Academy of Clinical Biochemistry Web site. Available at: http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1, 2003.
Using LT4 in those with IHD increases the risk of MI, aggravation of angina, or cardiac arrhythmias • For patients <50 years of age with underlying cardiac disease, initiate LT4 at 25-50 g/d with gradual dose increments at 6- to 8-week intervals • For elderly patients with cardiac disease, start LT4 at 12.5-25 g/d, with gradual dose increments at 4- to 6-week intervals • The LT4 dose is generally adjusted in 12.5-25 g increments Caution in Patients with Underlying Cardiac Disease Braverman LE, et al. Werner & Ingbar’s The Thyroid. A Fundamental and Clinical Text. 8th ed. 2000. Kohno A, et al. Endocr J. 2001;48:565-572. Synthroid® [package insert]. Abbott Laboratories; 2003.
Malabsorption Syndromes • Post-jejunoileal bypass surgery • Short bowel syndrome • Celiac disease • Reduced Absorption • Colestipol hydrochloride • Sucralfate • Ferrous sulfate • Food (eg, soybean formula) • Aluminum hydroxide • Cholestyramine • Sodium polystyrene sulfonate • Drugs That Increase Clearance • Rifampin • Carbamazepine • Phenytoin • Factors That Reduced T4 to T3 Clearance • Amiodarone • Selenium deficiency • Other Mechanisms • Lovastatin • Sertraline Factors That May Reduce Levothyroxine Effectiveness Braverman LE, Utiger RD, eds. The Thyroid: A Fundamental and Clinical Text. 8th ed. 2000. Synthroid® [package insert]. Abbott Laboratories; 2003.
Is There Any Role for T3 Supplementation in The Management of Hypothyroidism?
Congenital hypothyroidism (CH) is defined as thyroid hormone deficiency present at birth • It can occur because of an anatomic defect in the gland, an inborn error of thyroid metabolism, or iodine deficiency. • Diseases may manifest from birth or later Congenital Hypothyroidism (CH)
Incidence increased to about 1 in 2,000 due to more stringent screening strategies. • Incidence in Bangladesh1: 1,300, According to the research paper of 'Institute of Nuclear Medicine, Dhaka, Bangladesh'. • Male: Female = 1:2 Epidemiology
Classification Permanent Primary Secondary Peripheral Transient
Etiology of Congenital Hypothyroidism • Primary CH • Thyroid dysgenesis: 85% -agenesis, hypoplasia, ectopia • dyshormonogenesis- 15% • Resistance to TSH binding • Secondary (central) CH • TSH deficiencies • Congenital hypopituitarism (multiple pituitary hormone deficiencies) • Peripheral CH • Thyroid hormone • -transport defect • -metabolism defect • -Thyroid hormone resistance
95% -asymptomatic at birth • Some infants escape newborn screening, and laboratory errors occur, so pediatricians must still be alert for symptoms and signs of hypothyroidism if they develop. Clinical Manifestations..
Early Prolong gestation Large poteriorfontanelle Hypotonia Feeding / respiratory difficulty Delayed passage of meconeum Constipation Umbilical hernia Prolonged neonatal jaundice Hypotharmia • Late Coarse/puffy face Coarse hair Large Tongue Myxedema, Hoarse cry Hearing Impairment Speech delay Clinical Manifestations…..
Screening Technique • Specimen is blood spot in filter paper • Obtained by heel prick • and Cord blood Newborn Screening
Screening Protocols for CH: Three approaches re being used for screening: 1. Primary TSH, Back up t4 2. Primary T4, Back up TSH 3. Concomitant T4 and TSH
American Academy of Pediatrics Recommended Screening NICU/Preterm/Home delivery – 5 to 7 days of birth. Mother on thyroid medication/ Family history of CH – screen cord blood. For infants 1,500 g birth weight, repeat specimens should be sent at 2, 6, and 10 weeks of age due to the risk of delayed TSH elevation.
Preterm and low birth weight infants • Infants with trisomy 21 or cardiac defects have an increased risk of congenital hypothyroidism. • Monozygotic twins , if they are monochorionic, fetal hypothyroidism in the affected twin may get compensated by the normal twin through their shared fetal circulation. Who Needs Special Attention
A cord blood TSH value of >20 mIU/L can be used for the purpose of screening for congenital hypothyroidism. • For logistic angles, a higher cutoff of >30 mIU/L can be used.
Other relevant Investigation • Serum thyroglobulin • Anti thyroid antibody (TBG-AB)- In case of maternal autoimmune disease • CBC with PBF- anaemia (normo, micro and macro) • CXR- Cardiomegaly • ECG- bradycardia and low voltage ECG • CT Scan and MRI
New born screening CH? High TSH Low T4 High TSH Normal T4 Transient Hypothyroidism or permanent Hypothyroidism FT4, TSH again TSH > 20 MIU/L When To Start Treatment? TSH 6 -20 mIU/L: Repeat FT4, TSH weekly until normal, ≥10 mIU/L Persistently consider Rx TSH > 20mIU/L Start treatment soon, Further investigation to identify the cause
Treatment.. • Levothyroxine • The recommended dose of LT4 is 10-15 μg/kg/day given orally • Rapid normalization of thyroid function (ideally within 2 wk) is important in achieving optimal neuro-developmental outcome. • Levothyroxin must be ingested in the empty stomach, avoid soya, calcium and iron containing diet
CLINICAL FOLLOW-UP • Clinicalassessment of growth and development, should be performed every few months during the first 3 years of life. FOLLOW-UP