Download
1 / 9
100 likes | 412 Views
Hypothyroidism. Salma Akhter. I ncidence in the UK : 3.5 per 1,000 women and 0.6 per 1,000 men per year . Vague Symptoms: Exhaustion, Somnolence, Slow cognition, Intolerance to cold, Constipation, Depression, Weight gain, Calf stiffness, Menstrual

E N D
Hypothyroidism Salma Akhter
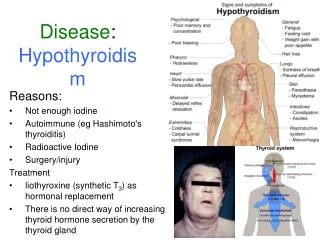
Incidence in the UK : 3.5 per 1,000 women and 0.6 per 1,000 men per year. • Vague Symptoms: Exhaustion, Somnolence, Slow cognition, Intolerance to cold, Constipation, Depression, Weight gain, Calf stiffness, Menstrual disorder, Carpal tunnel syndrome, Hearing impairment, Dry,thin,pale skin, Puffiness below eyes, Bradycardia, Slow relaxing tendon reflexes, Coarsening facial features, Pleural effusion, Pericardial effusion, Ascites, Non-pitting oedema of lower leg, Hyponatraemia, Hypercholesterolaemia, Impaired consciousness.
No Screening– but low threshold for doing TSH- esp over 60+s, Down’s Syndrome patients– should have TSH assay yearly as almost all go hypothyroid. Patients on Amiodarone, lithium and interferon. • The result should always be confirmed with a repeat sample. • Serum TSh has diurnal variation- lowest at 2 pm, highest at night time so ensure patient are always tested at the same time of the day
Diagnosis of Hypothyroidism • Overt hypothyroidism • TSH over 10 mU/l • FT4 below reference range • Subclinical hypothyroidism or mild thyroid failure • TSH 5 to 10 mU/l • FT4 normal • Secondary hypothyroidism • TSH low/low-normal • FT4 low
Thyroid Antibodies • It is worth testing for thyroid antibodies if a diagnosis of overt hypothyroidism is in doubt (TSH is just up- T4 normal or edging down) check only Thyroid peroxidase Ab, ( seen in 90% of autoimmune thyroiditis) checking thyroglobulin Ab offer no additional clinical Value, • If positive– treat if patient is symptomatic, patient euthyroid clinically, don’t treat & check TFT annually • If negative—, but if clinically hypothyroid– trail of treatment for 3 m
Treatment • The aims of treatment are simple: To make the patient feel well, and To keep the level of serum TSH in the lower half of the reference range: 0.4-2.5 mU/L • Serum TSH should be checked 8to 12 weeks after starting treatment and again the same time period after any dose adjustment, once stable- annually
Dose • Overt Hypothyroidism • Start on a full daily dose of 1.6 ug/kg (unless aged over 60 or history of ischaemic heart disease) Equates to 100µg daily for an average 60kg female, 125µg for a 75kg male • For any patient over 60 OR who has ischaemic heart disease Start low: 12.5-25 µg daily Note hypothyroidism-induced bradycardia may mask asymptomatic coronary heart disease so caution needed, Increase every 2-3 months in 25 µg increments until euthyroid2
When giving a trial of levothyroxine therapy for subclinical hypothyroidism, it is worth starting with close to a full replacement dose (around 75-100μg daily), it’s difficult to be sure symptoms might not be caused by hypothyroidism unless a therapeutic dose of levothyroxine has been tried.