Download
1 / 31
490 likes | 940 Views
Hospital acquired infections. Prof. Dr. Maha Al-Nuaimi. NCI .. HAI .. or Healthcare-associated infections. " nosus " = disease " komeion " = to take care of The very first requirement in a hospital is that it should do the sick no harm. What is NCIs (HAIs)?.

E N D
Hospital acquired infections Prof. Dr. Maha Al-Nuaimi
NCI .. HAI .. or Healthcare-associated infections. • "nosus" = disease "komeion" = to take care of • The very first requirement in a hospitalisthatitshould do the sick no harm
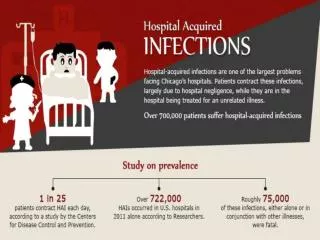
What is NCIs (HAIs)? • Infection in a hospitalized patient who was admitted for any other cause.. Not present or incubating on admission.. Occurring within IP, 2 up to 30 days after discharge. VIP of HAI: • 1/3rd of NCIsare preventable. • The CDC estimates: in US Annually. 2millioninfections. 99,000 deaths. • Norway – One of 19 patients admitted will develop a HAI • What about our hospitals? HAI Impacts: • Affects approximately 10% of all in-patients • Delays discharge • Costs two times more than if there is no infection • Direct cause of deaths: One death every 6 NCIs
Methicillin resistant Staphylococcus aureus, • Clostridium difficile, • Vancomycin-resistant Enterococcus and Legionnaires' disease.
Important 3 modes • Contact . • Droplet . • Airborne. • The 4 universal precautions: apply to: 1) blood; • 2) all body fluids, secretions, and excretions, except sweat, • 3)non-intact skin; and • 4) mucous membranes.
Risky groups • All hospitalized patients are susceptible • young children, the elderly, • Immuno-deficient and Transplant recipients.
What are the most common HAI? • The Commonest types are: • Urinary tract infection (UTI), • Surgical site infection (SSI). • Pneumonia (eg, ventilator-associated pneumonia [VAP]), • IV catheter Blood stream infection (BSI), • GIT infections • CNS infections.
Healthcare-Associated Urinary Tract Infection • Urinary tract infection (UTI) causes ~ 40% of hospital-acquired infections • What is the cause of UTI as NCI?? • 25% of inpatients are catheterized • Leads to increased morbidity and costs
Prevention of Catheter-Associated Urinary Tract Infection (CA-UTI) Avoid unnecessary catheterization Two main principles Limit the duration of catheterization
Indications for the use of indwelling urethral catheters Indications Perioperative use for selected surgical procedures Urine output monitoring in critically ill patients Management of acute urinary retention and urinary obstruction Assistance in pressure ulcer healing for incontinent residents Urinary incontinence is not an accepted indication for urinary catheterization 21 to 50 percent of urinary catheters not indicated Lo et al. (2008)Infect Control Hosp Epidemiol Suppl 1:S41-50
Is one catheter better than another? The concept: prevention of biofilm formation EM pictures of biofilms on silver coated catheters Morgan et al. (2009) Urol Res 37:89–93.
Intravenous catheter-associated bloodstream infections: incidence rates in ICUs: Germany: 2.1 per 1000 catheter-days 18 developing countries: 8.9 per 1000 catheter-days Edwards RJ. Am J Infect Control 2007; 35:290 – Gastmeier P. J Hosp Infect 2006; 64: 16 Pronovost P. N Engl J Med 2006; 355:26 – Rosenthal V. Am J Inf Control, 2008:36:627-637
Sources of the catheter-associated bloodstream infection Intraluminal from tubes and hubs Hematogenous from distant sites Extraluminal from skin Skin Vein
What are the Strategies to reduce IV catheter-associated bloodstream infections ?? Chlorhexidine gluconate-impregnated sponge
Chlorhexidine-gluconate impregnated dressings decreased major catheter-related infections: 1.40 per 1000 catheter-days Control dressings p=0.03 Cumulative Risk ChG dressings 0.60 per 1000 catheter-days Catheter-days Timsit JF. JAMA 2009; 301: 1231
Patient Age Burns Coma Lung disease Immunosuppression Malnutrition Acute shock Devices Invasive ventilation Duration of invasive ventilation Reintubation Medication Prior antiobiotic treatment Sedation Risk factors for Ventilator-Associated Pneumonia (VAP)
General precautions Staff education, hand hygiene, isolation, precautions: Avoid intubation and re-intubation. Prefer non-invasive ventilation. Prefer oro-tracheal intubation. Continuous subglottic aspiration Good oral hygeine, tracheostomy… Surveillance of infection and resistance; Adequate staffing levels as: Use sedation on and off., avoid paralytic agents, control DM ↓VAP by 51%
Strategies to prevent SSI • Objectives • Reduce the inoculum of bacteria at the surgical site • Surgical Site Preparation • Antibiotic Prophylaxis Strategies • Optimize the microenvironment of the surgical site • Enhance the physiology of the host (host defenses) • In relation to risk factors, classified as • Patient-related (intrinsic) • Pre-operative • Operative
Patient-related factors • Diabetes • Preoperative • Control serum blood glucose; reduce HbA1C levels to <7% before surgery if possible • Post-operative • Maintain the postoperative blood glucose level at less than 200 mg/dL • Smoking • Encourage smoking cessation within 30 days before procedure (Especially for cardiac surgery)
Procedure-related risk factors (preoperative) • Hair removal technique • Preoperative infection • Antimicrobial prophylaxis • Surgeon skill/technique • Asepsis • Operative time • Operating room characteristics
Antimicrobial prophylaxis • Administer within 1 hour of incision to maximize tissue concentration • Once the incision is made, delivery to the wound is impaired … why ??? • Duration of prophylaxis • Stop prophylaxis • within 24 hours after the procedure • within 48 hours after cardiac surgery • To: • Decrease selection of antibiotic resistance • Contain costs • Limit adverse events
1st principle of infection prevention at least 35-50% of all healthcare-associated infections are associated with only 5 patient care practices: • Use and care of urinary catheters • Use and care of vascular access lines • Therapy and support of pulmonary functions • Surveillance of surgical procedures • Hand hygiene and standard precautions
The 5 Standard prevention practices against NCI • hand hygiene. • personal protective equipment, which may include gloves, impermeable gowns, plastic aprons, masks, face shields and eye protection. the safe use and disposal of sharps. the use of aseptic “non-touch” technique for all invasive procedures, including appropriate use of skin disinfectants • routine environmental cleaning, • waste management& appropriate handling of fomites. • respiratory hygiene and cough etiquette • What is the most effective procedure for preventing infection?
The University of Geneva Hospitals (HUG), 8 years follow-up Rub hands… it saves money Pittet D et al, Inf Control Hosp Epidemiol 2004; 25:264
The University of Geneva Hospitals (HUG) « Talking walls »
Hand Washing VIP: • 80% of disease is spread by your hands. • Germs can live on dry surfaces for several hours and moist surfaces like, sinks for 3 days. • Hand Hygiene is the single most effective intervention to reduce the cross transmission of HAI infections. • Wear gloves (2 benefits).
“ 5 Moments for Hand Hygiene” Sax H, Allegranzi B, Uçkay I, Larson E, Boyce J, Pittet D. J Hosp Infect 2007;67:9-21