Download
1 / 23
• 230 likes • 561 Views
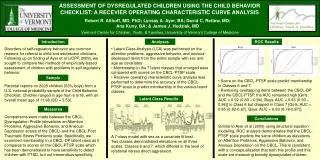
An Outcome Comparison of 3 Distinct Paddle Electrode Configurations of Thoracic Spinal Cord Stimulators for Chronic Neuropathic Pain. Angud Mehdi, BA Chengyuan Wu, MD, MSBmE David L. Penn, MS Ashwini D Sharan, MD Thomas Jefferson University Hospital Philadelphia, PA

E N D
An Outcome Comparison of 3 Distinct Paddle Electrode Configurations of Thoracic Spinal Cord Stimulators for Chronic Neuropathic Pain Angud Mehdi, BA Chengyuan Wu, MD, MSBmE David L. Penn, MS Ashwini D Sharan, MD Thomas Jefferson University Hospital Philadelphia, PA 16th NANS Annual Meeting Las Vegas, NV Sunday, December 9, 2012
Disclosure • No conflicts of interest for: • Angud Mehdi • David Pen • Chengyuan Wu • Dr. Sharan is a paid consultant for St. Jude Medical, and Medtronic Inc., however he has not received study support for this particular project.
Outline • Background • Methods • Results • Discussion • Conclusion
Background • Evidence suggests distinct lead configurations uniquely affect outcomes • 2 or 3 studies have been performed which compared percuntaneous and paddle electrodes(*North et al., Neurosurg Focus, 1997) • Studies have compared the effect of different programming parameters within one lead on outcomes (*Rigoard P., et al, Neurosurgery, 2012) • Our current study did NOT compare programming parameters • Tripole theory suggested that cathodal/anodal activation could shape electrical fields(*Linderoth and Meyerson, 1995 and Struijik and Holschemer, 1996)
Background • Evolution in electrodes to continue to provide field shaping and greater programming flexibility Courtesy of Medtronic Inc. Courtesy of Medtronic Inc. Courtesy of Medtronic Inc.
Hypothesis • Different paddle leads will have different clinical outcomes with respect to back and leg pain • Different paddle leads will have differences with respect to paresthesia and pain relief in the back and legs
Methods 5-column 3-column 2-column Courtesy of St. Jude Medical Courtesy of Medtronic Inc. Courtesy of Boston Scientific Note: These electrodes differ in the number of contacts, spacing of contacts, charge density, length, width, and programming flexibility.
Methods • Retrospective cohort study • Patients implanted January 2007 - August 2012 • Single institution (Thomas Jefferson University) • Identified 26 patients with > 3 months follow up
Methods • Data Collected • Specific system data/program parameters • Lead Location • Patient Outcome information • Owestry Disability Index (ODI) • Visual Analogue Scale (VAS) • Preoperative Pain Map • Postoperative Stimulation Map • Postoperative Pain Map
Methods • Our segmentation of the low back consisted of 9 regions defined by 4 surface landmarks. • Lateral aspect of 12th rib • Top of the iliac crest • PSIS • Gluteal folds
Results • 26 patients involved in final analysis • 11 5-column patients • 8 3-column patients • 7 2-column patients • Follow up: 501 + 355 days (146– 856 days) • 5-column: 413 + 162 days • 3-column: 596 + 443 days • 2-column: 588 + 476 days • Complications Final cohort(26) • 1 wound infections • 6 system revisions • 0 patient deaths http://wrcb.images.worldnow.com/images/9715482_BG1.jpg
Lead Location 5-column 3-column 2-column
Results 16
Summary • Electrode geometry appears to NOT affect VAS or ODI scores(p>.05) • Electrode geometry appears to affect distribution of paresthesia and pain relief distribution in back, buttock, legs, and feet regions
Discussion • Limitations of study design: • Retrospective • Small sample size • limits statistical analysis and ability to draw definite conclusions • Need for a future prospective study • Patients not randomized to a particular electrode • Outcomes may be distorted by selection bias • Need to test inter-rater reliability of our pain map • Need for control of stimulation programs and preoperative pain distribution
Conclusions • Trends observed: • 3-column electrode may be most effective in stimulating the low back from the 12th rib to PSIS • 5-column and 2-column electrode are similarly effective in stimulating the legs and feet • All electrodes equally effective in covering buttock/sacrum pain • 85% coverage of buttock pain • Greater pain reduction with more advanced electrode technology • 5-column is most consistent in pain reduction from low back to feet • All electrodes provided comparable reductions in VAS and ODI (p>0.05) • Need for a larger prospective study to elucidate preliminary findings
References • Buvanendran A, Lubenow TJ. Efficacy of transverse tripolar spinal cord stimulator for the relief of chronic low back pain from failed back surgery. Pain Physician. 2008 May-Jun;11(3):333-8. • De Andrés J, Quiroz C, Villanueva V, Valía JC, López Alarcón D, Moliner S, Monsalve V. Patient satisfaction with spinal cord stimulation for failed back surgery syndrome. Rev Esp Anestesiol Reanim. 2007 Jan;54(1):17-22. • Feirabend HK, Choufoer H, Ploeger S, Holsheimer J, van Gool JD. Morphometry of human superficial dorsal and dorsolateral column fibres: significance to spinal cord stimulation. Brain. 2002 May;125(Pt 5):1137-49. • Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J, Thomson S, O'Callaghan J, Eisenberg E, Milbouw G, Buchser E, Fortini G, Richardson J, North RB. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007 Nov;132(1-2):179-88. Epub 2007 Sep 12. • Linderoth, B. Meyerson BA. Dorsal column stimulation: modulation of somatosensory and autonomic function. Semin Neurosci. 1995;7(4):263-277 • Manola L, Holsheimer J, Veltink P. Technical performance of percutaneous leads for spinal cord stimulation: a modeling study. Neuromodulation. 2005 Apr;8(2):88-99. doi: 10.1111/j.1525-1403.2005.00224.x. • North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98-106; discussion 106-7. • North RB, Lanning A, Hessels R, Cutchis PN. Spinal cord stimulation with percutane- ous and plate electrodes: side effects and quantitative comparisons. Neurosurg Focus 1997;2:1-5 • .North RB, Kidd DH, Olin J, Sieracki JN, Petrucci L. Spinal cord stimulation for axial low back pain: a prospective, controlled trial comparing 16-contact insulated electrodes with 4-contact percutaneous electrodes. Neuromodulation 2006;9:56–67. • Rigoard P, Delmotte A, D’houtaud S, Misbert L, Diallo B, Roy-Moreau A, Durand S, Royoux S, Giot JP, Bataille B. Back Pain: A Real Target for Spinal Cord Stimulation? Neurosurgery. 2012 Mar;70(3):574-585. • Richter E, Sabo R, Garber J. Retrospective Data Collection Study to Evaluate Patients Implanted with a Novel 5-Column Paddle Lead. Poster presented at: Annual meeting of the North American Neuromodulation Society; Dec. 2-5, 2010; Las Vegas, NV. • Sankarasubramanian V, Buitenweg JR, Holsheimer J, Veltink P. Triple leads programmed to perform as longitudinal guarded cathodes in spinal cord stimulation: a modeling study. Neuromodulation. 2011 Sep-Oct;14(5):401-10; discussion 411. doi: 10.1111/j.1525-1403.2011.00383.x. Epub 2011 Aug 19. • Struijk JJ, Holsheimer J. Tranverse tripolar spinal cord stimulation: theoretical performance of a dual channel system. Med Biol Eng Comput. 1996;34(4):273-279 • Taylor RS, Van Buyten JP, Buchser E. Spinal cord stimulation for chronic back and leg pain and failed back surgery syndrome: a systematic review and analysis of prognostic factors. Spine (Phila Pa 1976). 2005 Jan 1;30(1):152-60. Review. • Wu C, Falowski SM, Sharan AD. “Spinal Cord Stimulation: General Indications." Neurostimulation for the Treatment of Chronic Pain, 1st Edition. Ed: Levy RM, Hayek SM, Deer TR. Saunders. September 2011. 22
Questions? 23