Download
1 / 11
110 likes | 278 Views
David Siegel, MD, PhD. Hackensack University Hackensack, New Jersey. Conventional Chemotherapy (CC) vs ASCT Randomized Studies. No. of pts 200 401 194 190 164 516. CR rate 5 vs 22** 8 vs 44** 6 vs 25** - 11 vs 30** 15 vs 17. Median EFS 18 vs 28** 19 vs 31** 16 vs 28**

E N D
David Siegel, MD, PhD Hackensack University Hackensack, New Jersey
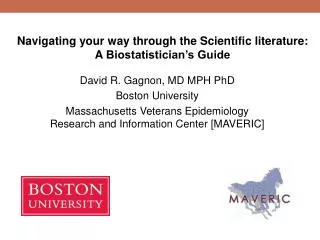
Conventional Chemotherapy (CC) vs ASCT Randomized Studies No.of pts 200 401 194 190 164 516 CRrate 5 vs 22** 8 vs 44** 6 vs 25** - 11 vs 30** 15 vs 17 MedianEFS 18 vs 28** 19 vs 31** 16 vs 28** 19 vs 25** 34 vs 42 21 vs 25 MedianOS 44 vs 57** 42 vs 54** 42 vs 58+** 45 vs 42 67 vs 65 53 vs 62 Age 65 65 50-70 55-65 65 - IFM90(N Engl J Med 96) MRC7(N Engl J Med 03) Italian MMSG(Blood 04) MAG 91(ASH 99) PETHEMA*(ASH 03) US Intergroup(ASH 04) CR=Complete Response EFS=Event-Free Survival OS=Overall Survival * Only in patients responding to initial CC ** Statistically significant Harousseau et al, Best Prac Res Clin Haematol. 2005;83-18
Age Not Important for Clinical Outcome on Multivariate Analysis • EFS P OS P Favorable cytogenics .004 Favorable cytogenics .009 ≤ 12 mo prior therapy .01 B2M ≤ 2.5 mg/L .03 B2M ≤ 2.5 mg/L .01 ≤ 12 mo prior therapy .4 Age < 65 yr .2 Age < 65 yr .8 EFS=Event-Free Survival OS=Overall Survival Siegel et al, Blood.1999; 9351-54
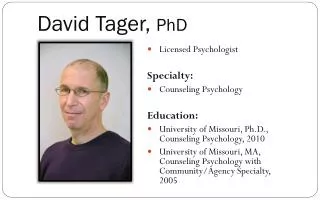
Event-Free Survival 1.0 Age N < 65 49 ≥ 65 49 0.8 0.6 Median =2.8 yrs Proportion 0.4 Median =1.5 yrs 0.2 p = .2 0 1 2 3 4 5 6 Years from first transplant Siegel et al, Blood.1999; 9351-54
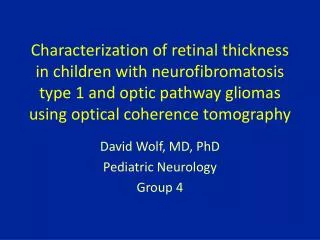
Overall Survival 1.0 Age N < 65 49 ≥ 65 49 Median = 4.8 yrs 0.8 0.6 Proportion Median =3.3 yrs 0.4 0.2 p = .4 0 1 2 3 4 5 6 Years from first transplant Siegel et al, Blood.1999; 9351-54
AggregateOS EFS,andCR DurationforPatients n=ReceivingAuto-SCT Over the Age of 70 Years* 1 Median (months) EFS 15 OS 24 CR duration 18 Probability 0.5 0 0 2 24 36 48 60 72 Months from first auto-SCT CR=Complete Response, EFS=Event-Free Survival, OS=Overall Survival * Median age was 72 years. Badros et al, BritishJournalofHaematology.-
What type of induction therapy would be best for this particular patient ? • Induction with high-dose pulse dexamethasone • (40 mg/m2 given on Days 1-4, 9-12, and 17-20 every 35 days)
What type of induction therapy would be best in a patient with more significant consequences of diabetes at baseline? • Weekly dexamethasone plus thalidomide in place of high-dose pulse dexamethasone at the outset • OR • Regimen combining dexamethasone with bortezomib
Recommendations • High-dose pulse dexamethasone for no more than 2 cycles • Stem cell harvest and ASCT • G-CSF, without cyclophosphamide • MEL-200 and proceed to autologous stem cell transplantation
Maintenance Therapy Following ASCT • No study in myeloma has yet shown a survival advantage
Pamidronate With or Without Thalidomide as Maintenance Therapy after Tandem Transplants • Longer progression-free survival (PFS) with addition of thalidomide • Significant benefits only in patients with • ≥ 90% response at randomization (P = .05) • Either deletion of chromosome 13 or B2M > 3 mg/L (P < .002) • Longer event-free survival • Overall survival similar in all 3 groups Attal M, et al. ASH 2004. Abstract 535.