Download
1 / 55
650 likes | 1.3k Views
cysticercosis. Zhao zhixin zxzhao@21cn.com The 3rd affiliated hospital of Sun Yat-Sen University. Key points. Pathogenesis and its relationship to clinical presentations Clinical presentations Diagnosis(imaging studies and biopsy)

E N D
cysticercosis Zhao zhixin zxzhao@21cn.com The 3rd affiliated hospital of Sun Yat-Sen University
Key points • Pathogenesis and its relationship to clinical presentations • Clinical presentations • Diagnosis(imaging studies and biopsy) • Treatment (Anti parasitic therapy and Symptomatic therapy)
Background • an parasitic disease caused by the pork tapeworm, Taenia solium • Infection occurs : tapeworm larvae enter the body and form cysticerci (cysts) • Encystment of larvae: occur in almost any tissue • the central nervous system (CNS) Involvement = neurocysticercosis (NCC) the most important manifestation present with dramatic findings
Pathogen • Taenia solium, causes disease in both pigs and humans depending on its developmental stage. • causes two forms of disease: • Taeniasis: adult tapeworm infection caused by ingestion of the adult form. Taeniasis occurs only in the human host. • Cysticercosis caused by cysticerciinfection in various organ systems can occur in both porcine and human hosts.
cysticercus • Surrounded by fibrous capsule • Containing an invaginated scolex • Bladder-like, fluid –filled cyst • Multiple,0.5-2cm in size
Pathogenesisand EPIDEMIOLOGY • Life cycle of t.solium • Where is the disease found? • Contagion summary • How NCC develop
Cysticer- cosis cysticerci Oncospheres Intestine Raw or undercook pork Ingested by pig and human Egg or gravid proglottides
Where is the disease found? • isfound worldwide. • rural, developing countries with poor hygiene • Places where pigs are allowed to roam freely and eat human feces- allows the cycle to continue.
Contagion summary(1): • Sources of infection persons with Taeniasis • Transmission ways not spread from person to person directly persons with Taeniasis will shed tapeworm eggs in their bowel movements
Contagion summary(2): • Infection can happen by By accidentally swallowing pork tapeworm eggs Through drinking contaminated water or food, by putting contaminated fingers to mouth
Contagion summary(3): autoinfection: • A person who has Taeniasis can reinfect himself. • internal autoinfection External autoinfection
HOW NCC develop ? Cysticercus survive in the brain disarming host defence, remain for years protected by brain-barrierasymptomatic Once the parasite degenerate Inflammatory response 80%cns parenchyma seizures numberous parenchyma cysticerki diffuse cerebral edema encephalitits 10-20% extraparenchymal: ventricles hydracephalus encased in a granuloma resolves scarring and calcification.
CLINICAL MANIFESTATIONS • symptoms can be different depending on where infection with cysticerci occurs how many the cysts are there • Most cases are asymptomatic. • Incubation: months~5ys
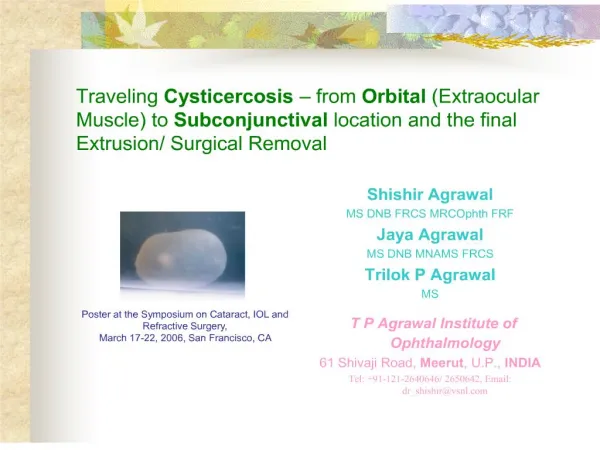
CLINICAL forms • Subcutaneous and Muscular involvement • NCC • Cardiac involvement • Ophthalmic involvement
Subcutaneous and Muscular involvement: • 2/3 of patients have nodules. • Number of nodules:1-1000 • Subcutaneous tissues: nodules on arms and chest. small, movable, painless • Muscular involvement: rarely painful; seen as calcifications following muscle bundles in thighs or arms. Massive parasite burden :limb muscular enlargement (pseudohypertrophy).
CLINICAL MANIFESTATIONS • Cardiac involvement: 1-5% of patients typically asymptomatic abnormal rhythms or heart failure (rare) • Ophthalmic involvement: (1-3% ). Intraocular cysts : solitary lesion freely float in the vitreous humor large parasitic burden : Visual disturbance and visual loss
NEUROCYSTICERCOSIS • NCC frequently asymptomatic. • Symptoms : similar to those found with other intracranial mass lesions consistent with elevation of ICP. • has gained increased recognition in the last 2 decades
NCC (1)Cerebral cysticercosis (2)Ventricular cysticercosis (3)Subarachnoid cysticercosis (4) mixed form: not common
NCC: (1)Cerebral cysticercosis 50 - 80% of NCC. Epilepsy (seizures) • Always the first and the only symptom. • Caused by cysticerci located in the Cortex near to the motorium. • characters: Multiple focal and unstable Neurosis: elevation of ICP: headache,vomiting ,visual disturbances
NCC: (2)Ventricular cysticercosis • 10% of brain cysticercosis • Caused by acute obstruction of CSF circulation • Manifests as :valve syndrome Intermittent positional severe headache,vomiting ,shock.
NCC: (3)Subarachnoid cysticercosis • 10% of brain cysticercosis • ¾ have increased ICP. Chronic ,intermittent meningitis. • CSF test: inflammation change
Focal neurologic deficits • are unusual • If positive: suggest alternative diagnoses tuberculoma tumor
Main Cysticercosis Diagnosis & Tests • lab test: Antibody test • imaging studies : Soft tissueX-rays brain CT scans MRI of brain • Procedures: Lumbar puncture: CSF tests Biopsyof the affective area subcutaneous nodule
Laboratory studies • Complete blood count (CBC):; • Serology ; • Stool for ova and parasites Lab studies : inferior to imaging in diagnosis but may play an adjunctive role.
Complete blood count (CBC): • Peripheral eosinophilia usually is not present • but eosinophils may be 10-15% of white blood cells (WBCs).
Serology-the most useful of lab tests. • Sensitivity :linked to number of parasitic lesions and the stage of lesions. • false-negative result: Single lesions calcification with parenchymal cysts • False-positive other parasitic infections high percentage of false positive for patients from endemic area (?30%)
Antibody test on CSF • performed on CSF: Sensitivity may be increased • it is only accurate when performed in patients with active meningeal disease.
Stool for ova and parasites • Positive: If with simultaneous intestinal tapeworm infestation • insensitive many samples needed over several days • nonspecific for T solium species as the eggs appear similar to those of the beef tapeworm.
Imaging Studies(1) Soft tissue x-ray • show calcifications of inactive cysts. • These may appear as oblong-shaped lesions.
Imaging Studies(2) CT scan • recommended as the first-obtained imaging study. • more widely available, less expensive, and has a faster imaging time than MRI. • Obtain contrast and noncontrast studies.
Imaging Studies(2) CT scan • Noncontrast study show 1.cystic lesions, or calcifications of inactive disease –the most common disease form at presentation 2.focal areas of edema in the acute phase 3. Findings indicate mass effect or hydrocephalus • Contrast study may depict nonenhancing cystic lesions ring enhancement signifying inflammation
Imaging Studies(3) MRI of brain • MRI is recommended as an adjunctive diagnostic tool to CT scan. • MRI may show a mural nodule within the cyst representing the larval scolex. This finding is pathognomonic. • MRI may show cysticerci within the ventricular system, which are often missed by CT scan due to the similar appearance of CSF and cystic fluids.
One Patient’s history • This 42y male presented to the emergency room with acute seizure • images from his head MRI show multiple low attenuation lesions; many with mural nodules; and multiple calcifications --consistent with active and chronic cysticercosis.
Lumbar puncture • insensitive and nonspecific in the diagnosis. needed only to exclude other diagnoses. • CSF is normal : in many cases • In the presence of significant inflammation: lymphocytosis, increased protein, and/or decreased glucose levels • eosinophilia With Special Wright or Giemsa stains a common but nonspecific finding
Biopsy Biopsy specimens may be taken from • subcutaneous nodules. Demonstration of organisms within nodular tissue is diagnostic of cystic • Biopsy of CNS lesions is rarely necessary.
diagnosis : • Signs and symptoms are nonspecific. • most patients do not present with definitive evidence of infection. • Diagnosis: by combining Epidemiologic data; clinical presentation; and Lab、imaging or Biopsy studies
diagnosis (1):Epidemiologic criteria Evidences of • Eating raw food habit or eating “rice meat” history or history of pass noodle like white gravid proglottides. • Individuals coming from or living in an endemic area • Household contact with an individual infected with T solium
(2)Absolute criteria • Histological demonstration of the parasite from biopsy • Direct visualization of subretinal parasites by funduscopic examination • Cystic lesions showing the scolex on CT scans or MRIs
(3)Major criteria • Lesions highly suggestive of NCC on neuroimaging studies CT scan or MRI showing • cystic lesions without scolex, enhancing lesions • typical parenchymal brain calcifications • antibodies: positive demonstrated by immunoblot assay • Treat response: Resolution of intracranial cystic lesions after therapy with albendazole or praziquantel
treatment • Emergency Department Care • Further Inpatient Care 1.Antiparasitic treatment 2.control therapy response 3.Symptomatic therapy 4.surgery therapy
Emergency Department Care: • seizure activity supportive care monitor, and correct metabolic abnormalities Anticonvulsants are effective. • evidence of increased ICP Steroids, osmotic agents, and/or diuretics • Initiate proper diagnostic procedures blood work and imaging. • Consult appropriate specialists neurosurgery, neurology, infectious diseases
1.Antiparasitic treatment medications • Anti parasitic therapy can only be done in the hospital • Common used medicines Albendazole Praziquantel -- Broad-spectrum anthelmintic
Albendazole • Adult Dose 18-20 mg/kg/d , bid/tid, for 10days • Pregnancy C - Safety for use during pregnancy has not been established.
Praziquantel • Adult Dose 20 mg/kg/d , tid , for 10days • Pregnancy B - Usually safe but benefits must outweigh the risks.
2.prevent inflammation after therapyCorticosteroids • A temporary increase in pericystic inflammation often is observed. • it is often recommended: be administered in combination with anthelmintic • This practice is controversial should be tailored to the individual patient according to the number and location of cysticerci
prevent inflammation after therapy • 20% Manitol: bid Dexamethasone:0.75mg bid • 1wk before till 1wk after the anti parasitic treatment course finished. 1w 10days 1w Manitol and DXM