Download
1 / 58
580 likes | 591 Views
Learn about immunostimulation, immunomodulation, and immunosuppression in treatments targeting the immune system with bacterial, cytokine, and antibody immunomodulators to combat autoimmune diseases and allergies.

E N D
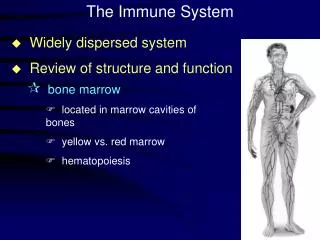
Therapies targeting the immune system: • Immunstimulation • Immunomodulation • Immunosuppression
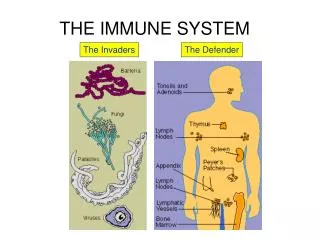
IMMUNOMODULATORS • modifying the immune system: either positive or negative • 1) Bacterial origin: • Freund adjuvant (CFA)-mycobacterium tuberculosis • human: BCG (bacillus of Calmette and Guerin strainof Mycobacterium bovis) – melanoma, carcinoma • Mf, T, B, Nk cells are stimulated, IL-1 secretion • muramyl dipeptide (bacterial cell wall proteoglycan) –less toxic • Staphylococcus aureus – superantigen – polyclonal activator of T cells • Escherichia coli heatlabile enterotoxin (LT), CT - adjuvant effect • Endotoxin: Gram negative bacteria outer cell wal– LPS • 2) Cytokines: rekombinant proteins (IL-1. IL-2, Epo) • cytokine antagonists: • signal inhibitors • soluble receptors: TNF, IL-1, IL-4 • 3)Antibodies:antibodies against cytokines or cytokine receptors, or any other membrane molecules • IVIG
Where to apply immunomodulation: autoimmune diseases, allergy • Causal treatment: • Tolerance induction: • Peptide immunization – e.g. SLE: DNA-mimotope peptides, • Inhibition of pathogen antibody production (autoreactive antibody or IgE) • Regulation of cytokine network • Regulation of signaling „ „ • Apoptosis based therapies
Immunomodulation by cloleratoxin-like enterotoxins Escherichia coli heatlabile toxin (Etx) A subumit: A1 (toxic ), A2 (adaptor) (ADP ribosilation, cAMP ,-> PKA Cl- out, H2O in ) B subunit (non toxic) - adjuvant pentamer ring, stabile non covalent bonds high affinity : KD= 7-5 x 1010 Receptor: GM1 (membrane raft) Effect: tolerance induction (auto-ag) adjuvant mucosal or systemic immunization
When and howcholera-likeenterotoxin is usedfortoleranceinduction? Diseaseantigenprepimmunization SRBC SRBC-CtxBp.o. BCG BCG-CtxBp.o. EAE (rat) MBP MBP-CtxBp.o.(ExperimentalAutoimmuneEncephalomyelitis - micemodel of multiple sclerosis) Diabetes insulinins-XCtxBp.o. (NOD mice) Arthritisnone ETXB s.c. Diabetes noneCTxBi.v., i.p (mucosalvaccination) Human: CTB – non-toxic, goodadjuvant, vaccinationagainstcholeraoralvaccine: inactivatedvibriocholera +CTB IgA, memory Inducingtolerancein HSP uveitis: mucosalimmunization tolerance (CTB-HSP peptideconjugates) small phase I/II trial in patients with Behcet’sdisease (BD) was undertaken with very encouraging results
The effect is based on interaction with receptors • Policlonal B cell activation • Without proliferation • Increased expression of: MHCII, B7, CD40, ICAM1, IL2Ra • therapy: local antibody production • TH1 –linked diseases: • autoimmune diseases • graft rejection Etx B subunit
Endotoxinexposition: effectonallergy and asthma Gram negative bacteria outer cell wall – LPS O-antigen: repeated O-polysacharides (glycan polimer) Immunostimulator: Lipid A conserved in different bacteria species Adjuvant effect -T memory IL-12, IFNg production In microbe-enriched environment Less asthma
Effect of LPS on IL-12 production of blood lymphocytes Similar effect on IFNg production TH1 shift, suppression of TH2 cytokines Prevention of atopy, diseases linked to atopy
Endotoxine induces TH1 response and suppresses TH2 reponse leading to allergy
Reverse correlation: between the incidence of microbial infections and allergy, asthma • Children exposed to haus dust, animals, non-pasteurized milk, low incidence of allergy • Big towns >>> villages: • Allergy • Frequent infections in the air trackt, stomach, gut • Higeny? „Hygiene hypothesis”
BUT: endotoxin is a double edges sward, may also induce asthma
2. Cytokines: • Recombinant proteins (IL-1. IL-2, Epo) • cytokine antagonists: IL-1RA signal inhibitors • Soluble receptors: TNF, IL-1, IL-4: • Specific, high affinity, • In vivo occurence • (due to proteolytic cleveage or alternative splicing) • Do not activate biol. response • Neutralises the ligands • Relative long half life • low/no immunogenicity
Cytokines: Immunomodulators effect application IFNa innate immunity up anti-tumor response upregulated IFNb „ „ IFNg adaptive immunity up „ „ protect against infections IL-2 activated killer cells anti-tumor effect IL-4 TH2 response up antibody production increases IL-10 TH1 response cellular toxicity decreases, autoimmune IL-12 TH1 response up cellular cytotoxicity up, anti-tumor Fas(CD95) CD8 cytotoxicity Thymus deletion, autoimmunity blocked TGFb helps wund healing, inhibit specific immune response decrease of immune response IL-1RA blocks IL-1R binding prevent septic shock, allergy GM-CSF WBC increase temporary neutropenia
TNF blocking therapy Very efficient according to several studies 2003 Albert Lasker AwardMarc Feldmann and Sir Ravinder Maini (Kennedy Institute, London) TNF blocking in RA and other autoimmune diseases .
Anti-inflammatory effects of anti-TNF-α therapy in rheumatoid arthritis The clinical course of 24 patients was followed for 4 weeks after treatment with either a placebo or a monoclonal antibody against TNF-α at a dose of 10 mg kg-1. The antibody therapy was associated with a reduction in both subjective and objective parameters of disease activity (as measured by pain score and swollen-joint count, respectively) and in the systemic inflammatory acute-phase response, measured as a fall in the concentration of the acute-phase reactant C-reactive protein.
3). Antibody mediated therapies • elimination of pathogen –hyperimmune sera (passive immunization) (rabies, hepatitis B, CMV, RSV, varicella/zoster) • Prevention of infection : RSV (respiratory syncytial virus) • Toxin neutralization- e.g. snake-bite, tetanus • inhibition of function: e.g. blood cloting (coagulation) • specific elimination of cells: e.g. anti-CD20elimination of CD20+ B cells • Targeting targeted therapies
Possible targets of antibodies: • Cell surface receptors • Cytokines and their receptors: • Graft versus host disease (GVH) • Malignant tumor • Immunosuppression • Inflammation • Trombocyte aggregation • Application of antibodies: • Diagnosis: detection of malignant cells - metastasis • Prognosis – detection of membrane markers • Hyperimmune antibodies : intramuscular, intravenal passive immunization • Anti-inflammatory therapies: autoimmune diseases, allergic diseases IVIG : Fcg R dependent • Peplacement therapies : immunodeficiency, autoimmune diseases
Polyclonal antibodies: • Non-antigen specific immunosuppression • SERA OBTAINED AFTER IMMUNIZATION OF ANIMALS WITH HUMAN CELLS • anti-thymocyte sera, anti-thymocyteglobulin: inhibits T cell response • anti-lymphocyte sera, anti-lymphocyte globulin • lymphopenia – against graft rejection or GVH • Problems: standardization, • selectivity: non-selective for T cells • non-self (animal protein) serum diseases • therefore:
Monoclonal antibodies: • homogenous • selective • Humanized or human antibodies – no immune response • Graft rejection: • anti-CD3: temporary elimination of T cells – but it may activate! • antibodies against cell surface proteins on APC and/or T cells immunosuppression CD4 or CD8 MHC II MHC I TCR T sejt CD3 ICAM-1 B7 LFA-1 CD28 IL-2 R CD40 CD40L APC • Non mitogenic anti-CD3 • Inhibition of costimulation: CTLA4-Fc • T cell depletion: anti-CD52 (Campath) • Antigen specific inhibition: ag/peptide • CD28 superagonist -Treg increases, but: „cytokin storm” • TNFa inhibition • Inhibition of cytokine and their receptors • Anti-inflammatory antibodies
Nature Reviews Cancer2; 750-763 (2002); doi:10.1038/nrc903LIGAND-TARGETED THERAPEUTICS IN ANTICANCER THERAPY < previousnext >
Bio-similar, bio-better, me-better • Biosimilar antibodies are “generic” versions of “innovator” (or “originator”) antibodies with the same amino acid sequence, but produced from different clones and manufacturing processes. • Bio-better antibodies are antibodies that target the same validated epitope as a marketed antibody, but have been engineered to have improved properties, e.g., optimized glycosylation profiles to enhance effector functions or an engineered Fc domain to increase the serum half-life • “Me better” antibodies with controlled and optimized glycosylation have been obtained in glyco-engineered CHO cells or yeast strains
Depleting antibodies specific for molecules expressed on B cell surface (CD20, CD22, and CD52). Monoclonal antibodies: Inhibition of factors/signaling pathways required for B cell survival, and activation (CD40/CD40L és BLyS/BR3 jelpálya) • AIMS: • maximum specificity : • targeting • neutralization • signalization • minimal immunogenicity: • humanized/humán antibodies • optimal effector function: • designed antibodies: • designed effector function: • ADCC - FcγR • CDC - C1q binding complement activation, • phagocytosis – FcγR, CR • antibody half life - FcRn
Antibody therapies- removal of self antibodies Plasmapheresis: about 50 % of plasma is removed (IgG 20 %, IgM ~50 %) remove immune complexes from circulation: autoimmune diseases: tissue specific IgG e.g. Goodpasture’s szindróma: antibodies against the basal membrane of lung, kidney glomeruli Myasthenia gravis (anti-acetilcholin receptor) Antibody overproduction: Waldenström macroglobulinemie –IgM hemolitic anemie: cold agglutinin IgM
Intravenal Ig therapy (IVIG) Immunomodulation, anti-inflammatory effect Application of IVIG therapie - examples • Neuroimmunological diseases : • demyelinization – Sclerosis multiplex- • Primer immunodeficiencies: Ig < 400 mg/dl • Idiopatic thrombocitopenia purpura: IVIG inhibits phagocitic removal of thrombocytes • CLL (chronic lymphacitic leukemie): against bacterial infections • infectious diseases, toxic shock (100 000/year) –sepsis • neutralizing, opsonizing antibodies, antibacterial antibodies, stimulating phagocytosis • Kawasaki disease: chronic vasculitis- IVIG - neutralizing effect, prevent coronary dilation
IVIG continue: • HIV- polyclonal B cell activation, high autoantibody level • specific antibody level is low • Parvovirus infection : DNA virus, erythroid precursors destroyed • anemie, reticulocytopenie • Transplantation: allo-antibodies suppressed • Neonatal alloimmune thrombocytopenie, • Immun thrombocytopenie
α2,6 syalic acide containing IVIG - model gyulladásgátló mediátorok α2,6 syalic acide recognizing receptor: SIGN-R, human: DC-SIGN-dendritic cells Anthony and Ravetch, J CLin Immunol. 2010.30 suppl. S9-S14
IMMUNOSUPPRESSION Where to use: to block pathological immune response - Allergy - Autoimmune diseases - Transplantation: graft rejection, GVH • a, Non-antigen specific • corticosteroids • CY-A, FK 506, Rapamycin, • irradiation • Cytostatic compounds • b, Antigen-specific (e.g. oral tolerance)
Antigen non-specific immunosuppression • Cortikosteroids • Inhibition of inflammation – inhibits pathological response • Mechanisms: acts via glucocorticosteroid receptors • Glucocorticosteroid (glucocorticoid, corticosteroid): • naturally occuring steroid hormone, 21 C atoms • a product of cholesterol metabolism • 90 % is bound to protein in vivo – corticosteroid binding globulin • >>5-8% bind to albumin -protects from degradation • Degradation: liver: keton group is hydrolysed, • 95 % excreted by kidney First drug: 1948: hydrocortisone (Rheumatoid arthritis )
CH2OH C=O CH2OH C=O CH2OH C=O CH2OH C=O OH OH OH OH The structure of the anti-inflammatory corticosteroid drug prednisone STRUCTURE: Synthetic products: OH cortisol prednisolon Cortisone Prednisone O O O O O Prednisone is a synthetic analogue of the natural adrenocorticosteroid cortisol. Introduction of the 1,2 double bond into the A ring increases anti-inflammatory potency approximately fourfold compared with cortisol, without modifying the sodium-retaining activity of the compound
Cell membrane steroid steroid receptor HSP-90 regulating gene element nucleus Mechanism of action cytoplasma nucleus transcription mRNS translation protein
Effect: • leucocyte circulation, number of neutrophils transiently increases, number of other cell types: decreases • change of function : enzime release • cytokine secretion: IL1, IL-2, TNF, IL-6 • lymphocyte activation, APC function • phagocytosis • anti-inflammatory effect: inflammatory cells’ function • metabolic effect: enhanced degradation of lipids, proteins, carbohydrates, • nucleic acids • toxicity Regulates expression of 1 % of the genes !
Non-steroid anti-inflammatory drugs • 400 BC • aspirin willow tree (Salix alba)- Hippokrates • Synthetic production:: XIX sz., USA –15x106 kg / year • Mechanism: • cyclooxigenase inhibitioninhibition of prostaglandin synthesis • enzime active site: serin acetilation (irreversible) • inhibition of bindin of arachidonic acid (reversible)
Phospholipid – cell membrane phospholipase A2 arachidonic acid 15 HEPTE lipoxin cyclooxigenase 15 lipoxigenase vasodilatation, PGH2 5 lipoxigenase LTB4 antagonizmus + FLAP TBX PGI PGE 5 HPETE vazodilatáció 5lipoxigenáz thrombocite LTA2 LTA4 szintase aggregation LTC4 szintáz LTB4 LTC4 transzpeptidáz muscle contraction PMN chemotaxis LTD4 permeability of veins PMN activation dipeptidáz cytokine production T cell ” LTE4 aszpirin
Cyclosporin (CsA) and FK506 acts in cytoplasm Bind to civlophilinhez (CyP), or FKBP CsA-CyP és a FK506-FKBP complexes bind to calcineurin, blocks [Ca2+] dependent activation inhibits activation of NF-Atc T cell activation NF-ATn synthesis, [Ca2+] [ Ca2+] activates calcineurin phosphatase , Dephosphorylated, activated NF-ATc goes to nuclei , binds to NF-ATn , active transcription factorÍ: NF-ATis formed Activation of gene transcription No activation of gene transcription
Effect of CsA and tacrolimus on the immune system T cells: selective effect on CD4+T helper cells IL-2, IL-3, IL-4 GMCSF, TNFa decreased decreased proliferation decreased Ca dependent exocytosis decreased apoptosis (AICD) B cells: decreased proliferation (no T cell help) decreased apoptosis Granulocytes: decreased Ca dependent exocytosis Rapamycin: similar to FK506, inhibits CD28 signaling, non Ca2+ dependent
Citotoxic compounds: Killdividing cells -act in the phase of DNA synthesis ( azatioprin, metotrexat), or -in all phases of cell cycle (cyclophosphamid) Specificity? Non-specific:UV, irradiation S-phase- specific (azathyoprin, metotrexate) Cell cycle specific (cyclophosphamid, chlorambucil) % antibody producing cells 100 - 10 - 1 - 0.1 - doses 24 h before antigen 24 h after antigen
The structure and metabolism of the cytotoxic immunosuppressive drugs azathioprine and cyclophosphamide. Inhibits purin biosynthesis (DNAsynthesis) DNA alkylating compound, non-stabile (all phases of cell cycle) The structure and metabolism of the cytotoxic immunosuppressive drugs azathioprine and cyclophosphamide. Azathioprine was developed as a modification of the anti-cancer drug 6-mercaptopurine; by blocking the reactive thiol group, the metabolism of this drug is slowed down. It is slowly converted in vivo to 6-mercaptopurine, which is then metabolized to 6-thio-inosinic acid, which blocks the pathway of purine bio-synthesis. Cyclopho-sphamide was similarly developed as a stable pro-drug, which is activated enzymatically in the body to phosphoramide mustard, a powerful and unstable DNA-alkylating agent.