Download
1 / 16
160 likes | 300 Views
The MONET trial: darunavir/ritonavir monotherapy shows non-inferior efficacy to standard HAART, for patients with HIV RNA <50 copies/mL at baseline.

E N D
The MONET trial: darunavir/ritonavir monotherapy shows non-inferior efficacy to standard HAART, for patients with HIV RNA <50 copies/mL at baseline JR Arribas, A Horban, J Gerstoft, G Fätkenheuer, M Nelson, N Clumeck, F Pulido, A Hill, Y van Delft, C Moecklinghoff, T Stark for the MONET Study Group Oral Late-Breaker presentation at 5th IAS Conference Cape Town, South Africa, July 2009 #TUAB106-LB
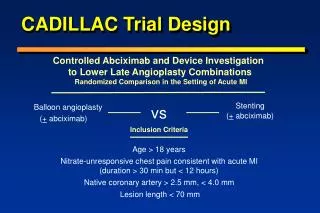
DRV/r 800/100 mg OD + 2 NRTI (re-optimised at baseline) n = 129 Follow-up phase 96 weeks 256 subjects No run-in period DRV/r 800/100 mg OD n = 127 Follow-up phase 96 weeks MONET - Trial Design • Taking 2 NRTI + either NNRTI or boosted PI at screening (stratified) • No prior use of darunavir (DRV) • HIV RNA <50 copies/mL for at least 6 months, • No history of virological failure 96 wks BL SC 30 days 4, 12, 24, 36, 48 weeks • Primary Endpoint:HIV RNA< 50 at week 48 (TLOVR). Per Protocol, Switch = Failure • 2 consecutive HIV RNA > 50 copies/mL (Roche Amplicor HIV-1 Monitor assay 1.5) • Stopping DRV/r • Starting NRTIs in the monotherapy arm • Stopping NRTIs in the triple therapy arm (switches in NRTIs were permitted at any time). J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET: Study Design and Objectives Primary objective: to show non-inferior efficacy for DRV/r monotherapy (800/100 mg OD dose) versus standard HAART (DRV/r + 2 NRTI). Study power: 80% to show non-inferiority for DRV/r vs DRV/r + 2 NRTIs, with a sample size of 125 patients per arm (delta = -12%). Analysis: Per protocol (PP): excluded patients with major protocol violations such as a history of virological failure, or patients randomised incorrectly (n = 10). Time to loss of virolgical response (TLOVR) Observed: only virological endpoints. Intent To Treat (ITT) – all randomised patients Switch = Failure (S = F) Switch Included (S F) All patients were followed up to Week 48
MONET: Baseline Characteristics (ITT) Age, years (median, range) Male (%) Caucasian (%) 43 (24-72) 83% 90% 43 (25-67) 78% 92% 579 12% 6.4 (4.0) 57% 43% 48% 28% 2 (1.6%) 14 (11.2%) 571 14% 7.4 (4.2) 56% 44% 35% 23% 1 (0.8%) 24 (19.0%) Disease characteristics CD4 count (median, cells/uL) CD4 <350 cells/uL (%) Duration of prior ARVs, years (mean, sd) Use of PI at screening (%) Use of NNRTI at screening (%) On their first NRTI combination PI naïve Hep B Surface Antigen, positive, n (%) Hep C Antibody, positive, n (%) DRV/r + 2NRTI (n=129) DRV/r (n=127)
MONET: Primary Efficacy Analysis:HIV RNA <50 copies/mL at Week 48, TLOVR, S = F Per Protocol analysis (PP) Intent to Treat analysis (ITT) Primary analysis • 1.6%; lower limit 95%CI: -10.1% • 1%; lower limit 95%CI: -9.9% 100 87.8% 86.2% 85.3% 84.3% 90 80 HIV RNA <50 by Week 48 (%) 70 60 50 40 30 20 10 0 DRV/r + 2NRTI (PP) DRV/r mono (PP) DRV/r + 2NRTI (ITT) DRV/r mono (ITT) N=129 N=123 N=123 N=127 Table EFF 4-5 J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET trial: sensitivity analyses Difference in 48 week HIV RNA response rate between DRV/r mono and DRV/r + 2NRTI arms (95% confidence intervals) Analysis -12% 0% -1.8% -7.0% +3.5% PP, HIV RNA <200, TLOVR, switch equals failure 94.8% vs 96.6% -1.6% +4.2% -7.4% ITT, HIV RNA <50, TLOVR, switch included(S F) 93.5% vs 95.1% -9.5% -3.2% +3.1% Observed HIV RNA <50 91.3% vs 94.6% -0.8% +2.6% -4.2% Observed HIV RNA <200 97.6% vs 98.4% DRV/r + 2NRTI better
MONET: Patient outcomes in DRV/r + 2 NRTI (ITT) Baseline DRV/r + 2NRTI: n=129 d/c or changed treatment, n=9 Missing data n=3 HIV RNA>50 x2: n=7 (TLOVR) Treatment period HIV RNA<50: 2 RNA <50 wk36: 1 HIV RNA<50: 110 HIV RNA<50: 6 HIV RNA>50: 1 HIV RNA<50: 8 no data: 1 Last visit HIV RNA<50: 97.7% 126/129
MONET: Patient outcomes in DRV/r monotherapy (ITT) Baseline DRV/r monotherapy: n=127 Missing data n=0 HIV RNA>50 x2: n=11 (TLOVR) d/c or changed treatment, n=9 Treatment period HIV RNA<50: 107 HIV RNA<50: 10 HIV RNA>50: 1 HIV RNA<50: 7 HIV RNA>50: 2 Last visit HIV RNA<50: 97.6% 124/127
MONET: Drug resistance Genotypic results DRV/r + 2NRTI N=129 DRV/r mono N=127 Patients with at least 1 successful genotype 13 22 No primary PI, DRV or NRTI mutations 21/22 (96%) 12/13 (92%) M184V 1 0 Primary IAS-USA PI mutations 1 1 DRV mutations 0 1 1 patient per arm had any evidence of genotypic resistance No patients had phenotypic resistance to DRV J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET: Median CD4 Cell Count (Observed) – ITT Median CD4 count: cells/uL DRV/r + 2NRTI (n=129) DRV/r mono (n=127) Time - weeks
MONET: Grade 2–4 drug related clinical adverse events Gr 2–4 AEs† ≥2% incidence, n (%) DRV/r mono DRV/r + 2NRTI (N=129) (N=127) GI (all AEs) 5 (3.9%) 7 (5.5%) Diarrhea 2 (1.6%) 6 (4.7%) Nausea 1 (0.8%)) 0 (0%) Rash (all types) 2 (1.6%) 2 (1.6%) †At least possibly related to study drug, excluding laboratory-related events J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET: Grade 3 / 4 Laboratory abnormalities (Worst values) > 2 % Incidence, n (%)* DRV/r + 2NRTI DRV/r mono n = 129 n = 126 ALT >5 x ULN 2* (1.6%) 6* (4.8%) AST >5 x ULN 1 (0.8%) 6* (4.0%) Lipase >3 x ULN 3 (2.3%) 4 (3.2%) Total cholesterol >7.77 mmol/l, sustained 2 (1.6%) 6 (4.8%) * 7 of the 8 cases of ALT and AST elevations were associated with Hepatitis A or C co-infection J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
Conclusions • Darunavir/ritonavir monotherapy showed consistently non-inferior efficacy versus triple antiretroviral drug treatment at Week 48. • Most elevations in HIV RNA were low level (50-400 copies/mL), and patients were re-suppressed <50 copies/mL at last visit, either on the original randomised treatment or with intensified treatment. • There were no patients with phenotypic resistance to darunavir during the trial – one patient per arm showed at least one genotypic PI mutation. • No new or unexpected safety signals were detected (details submitted to EACS and AELD conferences). J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
Efficacy of darunavir/ritonavir as single-drug maintenance therapy in patients with HIV-1 viral suppression: a randomized open-label non-inferiority trial, MONOI-ANRS 136 C. Katlama et al #WELBB102 WEDNESDAY. LATE BREAKERS TRACK B. Session Room 1. 13:10 J. Arribas et al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET: Acknowledgements Thanks to all the 256 patients who participated in the MONET trial, plus the investigators and study monitors
MONET: Acknowledgements Participating centers: Austria: A. Rieger, N. Vetter Belgium: N. Clumeck, E. Florence Switzerland: P. Vernazza Germany: G. Fätkenheuer, A. Stoehr, W. Schmidt, M, Stoll, C. Stephan Denmark: J. Gerstoft, C. Pedersen, L. Mathiesen Spain: B. Clotet, F. Pulido, J. Arribas, J. Gatell, J. Iribarren, R. Rubio, J. Pasquau United Kingdom: M. Johnson, B. Peters, M. Nelson, A. Winston, Hungary: D. Banhegyi Israel: S. Maayan Italy: A. Lazzarin, A. Antinori, F. Suter, A. D‘Arminio Monforte, G. Carosi Poland: A. Horban Portugal: F. Antunes, R. Marques Russia: N Zakharova, V. Pokrovsky The authors would like to thank the patients and their families for their participation and support during the study, and the MONET study team and co-investigators for their collaboration. This study was sponsored by Tibotec, a division of Janssen-Cilag.