Download

1 / 64
640 likes | 813 Views
Acute Rheumatic Fever ( Licks the Joints and Bites the Heart). Etiology: Group A beta hemolytic streptococci (GABS) Serotypes (M protein..,3,18) Rheumatogenicity. Epidemiology : 5-15 y/o Developing or underdeveloped countries New outbreaks Crowding Low sanitary Season

E N D
Acute Rheumatic Fever(Licks the Joints and Bites the Heart) Etiology: • Group A beta hemolytic streptococci (GABS) • Serotypes (M protein..,3,18) • Rheumatogenicity
Epidemiology: • 5-15 y/o • Developing or underdeveloped countries • New outbreaks • Crowding • Low sanitary • Season • Pharyngitis but not impetigo
Pathogenesis: • Unknown • Toxic effect • Abnormal immune response • Genetic influence (alloantigen on surface of non T-lymphocytes in 99% of ARF but 13% of controls)
Pathogenesis: Abnormal immune response • Alteration in helper and suppressor T cells • Anti heart antibodies • IgG, IgM, C3 deposition in pericard
Streptococcal and Human Tissue Immunologic Cross Reactivity • Capsule • Hyaluronic acid • Cell wall • M – protein • Group carbohydrate • Rhamnose • N-acetyl glucosamine • Protoplast membrane • Protein, lipid, glucose Joint Myocardium Valves Myoc.Sarcolemma, Subthalamic & Caudate nuclei
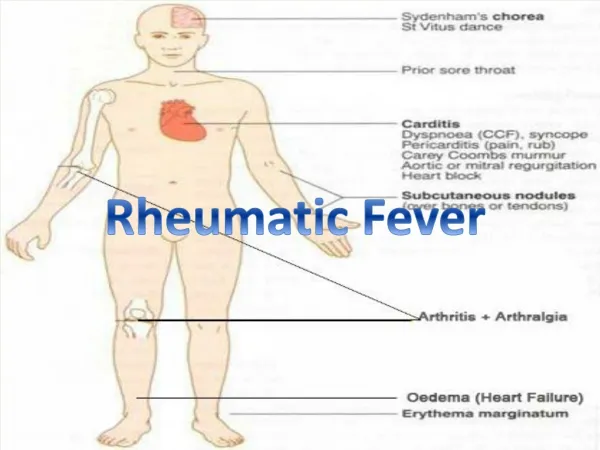
Clinical manifestations: • Polyarthritis: • The most common • Migratory polyarthritis • Tenderness • Large joints • Duration • Joint effusion and analysis • Response to ASA • There is often an inverse relationship between the severity of arthritis and the severity of cardiac involvement.
Poststreptococcal Reactive Arthritis: • Arthritis and recent evidence for GABS infection but do not fulfill the Jones criteria • Arthritis course & response to Rx. like JRA • About 5% acquire valvular disease without secondary prophylaxis
Clinical manifestations: • Carditis: • 40-80% • Mitral valve (the most common) • Pancarditis • Pericarditis • Arrhythmia • CHF
Subclinical Carditis: • >90% • ? Over diagnosis
Age: Carditis < 3 Y/O 90% 3-6 Y/O 50% 14-17 Y/O 32% > 25 Y/O Rare The Incidence of Carditis Depends on Age:
Carditis: • Isolated Mitral valve disease has 76% rheumatic etiology • Isolated Aortic valve disease has 13% rheumatic etiology • Combined Mitral and Aortic valve disease has 97% rheumatic etiology Roberts: in Moss & Adams textbook, 2001 edition
First streptococcal pharyngitis attack cause ARF in: Epidemic = 3%, Endemic = 0.3% • Second attack cause ARF in 11- 65% (after 10 years 4-8%) • RHD and cardiomegaly has 43% recurrence rate • RHD and no cardiomegaly has 27% recurrence rate • Normal heart has 10% recurrence rate • < 5% have chronic active carditis for > 6 months duration • Rheumatic activity may be prolonged with rebound
Clinical manifestations: • Sydenham chorea: • Deterioration of handwriting • Emotional instability • Milkmaid’s, silk fork and bag of worm signs • Late presentation • Disappear with sleep
Clinical manifestations: • Subcutaneous nodule: • Not tender • Extensor surface • Associated with severe carditis (MS)
Clinical manifestations: • Erythema Marginatum: • Not pathognomonic • Non tender • No itching • Associated with chronic carditis
Minor Manifestations: • Fever • Arthralgia
Modified Jones criteria: • 2 major • or one major and 2 minor criteria plus evidence for recent streptococcal infection. Recurrence of ARF: • Only one major criteria • or fever, arthralgia, • and elevated acute phase reactants plus evidence for recent streptococcal infection.
Lab findings: • ASO titer (acute and convalescent sera) • ADB • AH • Throat culture • ECG • Echocardiography
Frequency of Elevated Antibody Titer (%) in Patients With ARF
Antibody response: • Anti-A carbohydrate test reaches a peak 1 month after GABS infection and declines to normal levels about 2 years thereafter, except in patient with persistent rheumatic MR which will be maintained for several years.
Frequency of Positive Throat Culture Following Untreated Streptococcal Pharyngitis
Differential diagnosis: • JRA • SBE • Connective tissue disorders
Treatment: • Penicillin • ASA (first sign of toxicity is hyperventilation) • Prednisolone • Rx. For CHF • Bed rest • Rx. Of Chorea (Phenobarbital (is choice) 16-32 mg every 6-8 hr PO, chlorpromazine 0.5 mg/kg every 4-6 hr PO, diazepam, haloperidol 0.01-0.03 mg/kg/24 hr divided bid PO, valproate, vitamine E 50 mg/2 wk) • SBE prophylaxis (not penicillin)
Patients with typical migratory polyarthritis and those with carditis without cardiomegaly or congestive heart failure should be treated with oral salicylates. • The usual dose of aspirin is 100 mg/kg/day in 4 divided doses PO for 3-5 days, followed by 75 mg/kg/day in 4 divided doses PO for 4 wk. • There is no evidence that nonsteroidalantiinflammatory agents are any more effective than salicylates.
Patients with carditis and cardiomegaly or congestive heart failure should receive corticosteroids. • The usual dose of prednisone is 2 mg/kg/day in 4 divided doses for 2-3 wk followed by a tapering of the dose that reduces the dose by 5 mg/24 hr every 2-3 days. • At the beginning of the tapering of the prednisone dose, aspirin should be started at 75 mg/kg/day in 4 divided doses for 6 wk. • Supportive therapies for patients with moderate to severe carditis include digoxin, fluid and salt restriction, diuretics, and oxygen. • The cardiac toxicity of digoxin is enhanced with myocarditis.
Surgical Treatment: • MR: • Functional class III or IV • LVSD >26 mm/m2 • LVDD >40 mm/m2 • SF < 31% • AI: • Functional class III or IV • LVSD >55 mm • lower limit of normal SF & EF
Prevention: • Primary prophylaxis • Secondary prophylaxis • 3 or 4 weeks 600.000-1.200.000 units Benzathine Penicillin • No vaccine available
Duration of secondary prophylaxis?AHA 2009 Rheumatic fever without carditis 5 yr or until 21 yr of age, whichever is longer. Rheumatic fever with carditis but without residual heart disease (no valvular disease) 10 yr or until 21 yr of age, whichever is longer. Rheumatic fever with carditis and residual heart disease (persistent valvular disease) 10 yr or until 40 yr of age, whichever is longer, sometimes lifelong prophylaxis
Immunologic Factors in Patients With Acute Rheumatic Fever Compared to Patients With Rheumatic Heart Disease and Healthy Individuals. Sabri MR, Zohouri D, et al, IJMC; 2001; 26(3,4) :116-119
Aim: To clarify the state of different immunologic factors in patients with ARF and RHD in compare to the healthy individuals. • Patients and Methods: ARF (21 patients), RHD (19 Patients), and. healthy children as the control group (20 children) were studied. All patients were evaluated and followed for the presence and the severity of carditis, heart failure, and valvular involvement with echocardiography. ASO titer, ESR, serum C3 and C4, IgA, IgM, and IgG, IgM Rheumatoid Factor (RF), IgM and IgG anti-cardiolipin antibody (ACLA), and IgM and IgG anti-M group A streptococcal protein (AMP) were compared.
Results: 1) A significant difference for IgG and IgM ACLA between groups. These significances were shown to reflect the difference between patients with ARF and the other two groups. 2) A significant difference for IgG AMP between ARF and RHD groups. 3) A significant difference for IgM RF between ARF and RHD groups. 4) A significant difference for serum IgG between groups. This significance was shown to reflect the difference between patients with ARF and the two other groups. 5) Serum IgG was significantly lower in patients with than in patients without aortic valve involvement. Similarly, Serum IgG was significantly lower in patients with pericardial effusion.
Conclusion: There are significant differences for IgG and IgM ACLA and IgG AMP and serum IgG levels and IgM RF between ARF patients and the other two groups. The reproducibility of finding as well as whether IgG has a “protective effect” in patients with ARF preventing them from developing pericardial effusion, aortic valve involvement, or other complications are notable questions that must be answered in larger studies.
Correlation Between The Severity of Carditis And The Level of Acute Phase Reactants and Anti Streptolysin O Titer In Acute Rheumatic Fever, A Retrospective Study In Shiraz, Iran. SABRI MR, KADIVAR MR; MJIRI, 1999; 13 (1); 11-14
Frequency of the Observed Symptoms and Signs in the Study Group (104 Patients).
Frequency of the Echocardiographic Findings in the Study Patients
Results: • The ESR was 20 Wintrobe unit in 98.0%. • The CRP was elevated in 83.0%. • The ASO titer was 400 Todd unit in 91.0% of patients. Conclusion: • There was no significant statistical difference between those patients with mild and severe carditis for the level of ESR, CRP, and ASO titer. • There was also no significant statistical difference between the level of these parameters and the presence or absence of carditis, and the patient’s age (8 years or >8 years old).
A Prospective One Year Follow Up of Patients With Acute Rheumatic Fever And Evaluation of Valvular Regurgitation SABRI MR, REZAIE M, 13 th International Congress Of Geographic Medicine and the Congress of cardiovascular diseases , 2-5 Oct. 2000 Shiraz-Iran
Introduction: Initial carditis, cardiomegaly, CHF, moderate or severe degrees of valvar regurgitation and recurrence of ARF significantly increase the risk of subsequent rheumatic heart disease. Patients and methods: In this study, 80 children with first attack or recurrence of ARF associated with carditis were visited a by pediatric cardiologist and echo was done for them. 64 patients had regular follow up for one year.
Results: • Valvular regurgitation disappeared in seven patients (11%) at the end of follow up. • Severity of MR and AI decreased in 74% and 61% of patients respectively after one year. • In isolated MR, the regurgitation decreased in severity in 53.3% of patients and there was no significant statistical difference between this group and those who had 2 or more valvar regurgitation ((p=0.37). • 4) There was no significant statistical differences between two sexes (p=0.40), in different age groups (p>0.30) and type of presentation at the initial attack of ARF (carditis+arthritis or chorea or both with p>0.70).
Results: • Mitral valve involvement in patients with CHF was more severe than in patients without it. • Decrease in the severity of valvular disease was more significant in patients without CHF. • There were no statistical difference between patients with respect to initial ASO titer, ESR and CRP level. • There were no statistical difference between patients who received anti-inflammatory medication during acute phase of disease, comparing with those who didn’t (all p>0.05). • 5) Six patients had recurrence of ARF and all of them had no change in valvular involvement at the end of one year follow up.
Serum Penicillin Level After Intramuscular Injection of 1.200.000 Units of Benzathine Penicillin G, in Children With Rheumatic Fever. SABRI MR, KADIVAR MR, BORZOUEE M; MJIRI; 2000; 14 (1); 23-26
Patients and Methods: • 42 patients with RF • Mean age ± SD = 14.8 ± 11.9 years • SPL was determined by disk agar diffusion method • The minimum accepted SPL to be effective against group A hemolytic streptococci was 0.02 µg/ml