Download
1 / 67
670 likes | 890 Views
Osteoarthritis in Active Persons September 2012. Kevin deWeber, MD, FAAFP, FACSM Director, Primary Care Sports Medicine Fellowship Uniformed Services University Bethesda, MD. Objectives: to discuss…. Diagnosis of Osteoarthritis Risk factors for Osteoarthritis

E N D
Osteoarthritisin Active PersonsSeptember 2012 Kevin deWeber, MD, FAAFP, FACSM Director, Primary Care Sports Medicine Fellowship Uniformed Services University Bethesda, MD
Objectives: to discuss… • Diagnosis of Osteoarthritis • Risk factors for Osteoarthritis • Treating active persons with Osteoarthritis
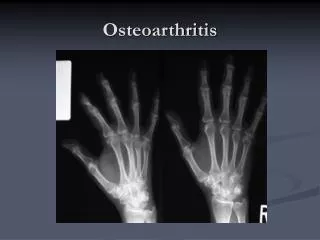
Definition of OA Disease of the joints characterized by: • Progressive articular cartilage loss • New subchondral bone formation • New bone and cartilage formation at joint margins • Low level synovitis & PAIN!
Clinical Diagnosis • Joint Pain • Typical Pain Pattern • Xray Findings • Standing films • AP with 30 deg flexion • No Sign of Zebras
Pathogenesis of OsteoarthritisAn Interplay of Factors Dieppe, American Academy of Orthopaedic Surgeons, 1995
Articular Cartilage • Chondrocytes • Extracellular matrix • Water (80%) • Collagen fibers • Proteoglycans
Core Protein Hyaluronic Acid Link Protein Glycosaminoglycans Proteoglycan Aggregate Proteoglycan aggregate Proteoglycan monomer
Articular Cartilage • The Living Sponge • Shock Absorption = Water Content + Glycosaminoglycan • Limited Supply!! One Time Offer!!
Core Protein Hyaluronic Acid Link Protein Glycosaminoglycans e.g. Chondroitin sulfate, Keratan sulfate (polysaccraride chains containing GLUCOSAMINE) Proteoglycan aggregate
Pathogenesis in OA • Decreases in: • GAG synthesis • Size of Aggregates, GAG & Hyaluronic acid • Collagen x-linking • Water content • Traumatic damage
Core Protein Hyaluronic Acid Link Protein Glycosaminoglycans Pathogenesis of Osteoarthritis Structure of Cartilage Proteoglycan Decreased Synthesis
Epidemiology of OA • In U.S. by age 30 • 3% symptomatic OA • In U.S. by age 60 • 40% report pain from OA • 80% radiographic evidence of OA • 100% histologic evidence of OA Felson, Annals Int Med, Oct 2000 Loeser, Rheum Dis Clin North America, Aug 2000
Risk Factors for OA Systemic Risk Factors Joint Biomechanical Risk Factors Joint trauma Obesity (knee, hip, hand) Occupation Abnormal joint biomechanics Dysplasia, malalignment, instability, abnormal innervation Knee extensor wkness Sports w/ joint risk • Age • 10-fold increase from 3065 • Genetics (generalized) • Gender • Men <50: higher risk • Women >50: higher risk • Nutritional • Low vitamin C and D intake
50% decrease in OA with with 11# wt loss Larger effect in women (Felson et. al. Ann Int Med 1992, Framingham Heart Cohort data) Strong Risk Factor for OA Obesity
Strong Risk Factor for OA Joint Trauma • Odds Ratio = 4.20 in meta-analysis • O.R. = 5.95 for major injuries (tendon/ligament, fractures, meniscal) • O.R> = 3.12 for unspecified injuries • Muthuri et al, Osteoarthritis Cartilage 2011
Moderate Risk Factor for KNEE OA Certain Vocational Activities • Meta-analysis pooled odds ratio for knee OA = 1.61 • Kneeling/bending, “heavy work,” lifting, carrying, climbing stairs, and “elite sports” • McWilliams et al, Osteoarthrits Cartilage 2011
Soccer and OARetrospective data • Lindberg et al: 4.5x prevalence of Hip OA in elite players • Shepard et al: 10x prevalence Hip OA (13% vs 1.5%) in ex-pro’s • Drawer et al: 32% prevalence lower-limb OA in ex-pro’s • Roos et al: 4x prevalence in pro’s • 16% vs 4.2% in amateur, 1.6% control
What other activities increase risk of HIP OA? • Heavy lifting • 10-20 kg x 10-20 years • Jensen LK. Occup Envir Med 2008 • Farming (as above) • “Sporting Activities” carries OR of 2.0 • Lievense AM et al. Arthritis Rheum 2003
Is physical activity a risk factor for knee or hip OA? • Wang Y et al, 2010 J Rheumatol • Prospective cohort, n=39,023 • KNEE: + risk (esp. vigorous activity) • HIP: no risk • Urquhart DM et al, 2011 MSSE • Systematic review • KNEE only • Conflicting evidence • MORE tibialosteophytes • LESS jt space narrowing • MORE cartilage volume
Does Running Cause Osteoarthritis? We don’t know conclusively! (but there are some associations…)
+ HIP Influence of sporting activities on the development of OA of the hip: a systematic review. Arthritis Rheum 2003 Apr;49(2):228-36 Lievense AM et al • Running: 10 studies reviewed • “Moderate” evidence of positive association between running and hip OA • >3 high-quality case-control studies w/ consistent findings • Odds Ratio 1.7 – 12.4
+ Is Excessive Running Predictive of Degenerative Hip Disease? British Medical Journal 1989 Marti B at al • Elite distance runners, bobsledders, & controls • Increased hip OA in runners’ xrays • O.R. 12.4 • Age, mileage, & running pace predictive of OA • Signif. more OA in those running >60 mi/week
What sports increase risk of Shoulder Osteoarthritis? • Increased risk of glenohumeral OA in elite tennis players in one small study • Maquirriain J et al. Brit J Sports Med 2006
Questions to ask your patients who want to run “Are your joints currently normal?” “What other risk factors do you have for OA?”
Running has significant benefits Less obesity Less diabetes Less heart disease Less depression Better bone density Moderate running on normal joints is healthy Too much of any good thing can be bad What to tell your patients who want to run
High risk of OA: Obesity Traumatic joint injury Moderate risk of OA High impact sports Heavy labor Running > 60 mi/wk ? Competitive weight lifting What To Tell Your Patients
Prior LE fracture, dislocation, major ligament or meniscal injury: Higher risk of OA Advise low-impact exercise If run, <25 mi/wk Obese patients Lose weight however you can! Joint instability, incongruity, loss of innervation: Advise low-impact exercise Patients needing caution when considering running
32 yo male stockbroker R knee pain for 9 mos h/o “old football injury” Swells after playing softball No locking or giving way Neg PMHx & PSHx No fevers, rash, other joint pain Case Study
Case Study (cont) Exam • Full ROM • Mild effusion • Mild medial joint line ttp • Neg McMurray/Thessaly • No ligamentous laxity
Treatment of Osteoarthritis Overview • Nonpharmocologic Measures • Education, Weight loss, Exercise, & Bracing • Pharmacologic Measures • Analgesics, Glucosamine, Injectables • Alternative Therapies • Acupuncture, Magnets, Balneotherapy, Thermotherapy • Surgery
Zhang W et al.OARSI recommendations for the management of hip and knee osteoarthritis Part III: changes in evidence following systematic cumulative update of research published through January 2009.Osteoarth and Cartilage 2010; 18:476-99.
Level of Evidence (LOE) • LOE 1a: meta-an • LOE 1b: RCT • LOE 2: cohort study • LOE 3: case series • LOE 4: expert opinion
Educate Your Athletes • Objectives of treatment • Changes in lifestyle • Importance of exercise • Pacing yourself • Weight reduction if needed • Unloading of joints
Lose Weight if Overweight/Obese(LOE 1a) • 5% wt reduction goal • Break that vicious cycle: • Team approach is critical
Evidence for Benefit fromExercisein Treating Knee and Hip OA • Regular aerobic walking for (Ia) • Home-based quad strength exercises (Ia) • Water-based aerobic exercise (Ia)
What Kinds of Exercise are OK? • Little evidence-based recommendations • Common sense advice • Avoid further trauma • MINIMIZE RUNNING • Wise to avoid high-risk activities • Listen to your joints X
Knee Bracing(LOE 1a) • Medial or lateral unloading
Lateral Wedge Insoles(LOE 1a for knee) • Medial tibio-femoral OA
Other Effective Therapies • TENS effective in some with knee or hip OA • Short-term, 2-4 weeks • Acupuncture relieves pain • Heat/Ice thermotherapy (Ia knee) • Balneotherapy (Ia knee)
Oral Therapy No disease modifying drug for OA (yet) • Tylenol, max 3-4 gm/day • analgesic of choice • LOE 1a, but small pain relief if OA mild/mod • NSAIDs—LOE 1a • Tramadol: LOE 1a in short-term trials • No long-term trials • More side-effects than Tylenol • Glucosamine sulfate
A Few Words about NSAIDS • 2x effective as Tylenol • Much more frequent/serious side effects • Reserve for inflammatory flare-ups • Use lowest effective dose • Avoid long-term use; protect GI tract if must • COX-2 vs Non-selective: • Lower GI risk, but not zero
Core Protein Hyaluronic Acid Link Protein Glycosaminoglycans e.g. Chondroitin sulfate, Keratan sulfate (polysaccraride chains containing GLUCOSAMINE) Glucosamine: Mechanism of Action • Stimulates chondroitin synthesis • Small anti-inflammatory effect
Glucosamine in Knee and Hip OA • LOE 1a for moderate pain reduction • Significant differences in results between preparations (G. sulfate more effective) • LOE 1a for preservation of joint space • 1500 mg/day • One obsvnl study: reduced rate of joint replacement • 6% vs 14%
Chondroitin in Knee OA • Effective for pain (Ia) • LOE 1a for preservation of joint space • 800 mg/day
Glucosamine/Chondroitin--My Take • I recommend in ALL patients with knee and hip OA • GS 1500 mg/ CS 800 mg • 3 month trial, evaluate efficacy; continue if helping • Consider indefinite use even if no pain relief for joint space preservation
Miscellaneous Herbals • ASU: Avocado-Soybean Unsaponifieds • Oils that remain after hydrolysis • Blocks TNF-α, COX-2 • Improved pain & function, knee & hip (Ia) • More effective than acet, similar to NSAIDs • Rosehip: Ia for pain, knee & hip • SAM-e NOT effective
Topical Treatments:Useful as Adjuncts • Topical NSAIDs • LOE 1a for pain, stiffness, function • As effective as oral; safer • Side effects = placebo • Onset slightly slower than oral • Duration?? • Capsaicin • LOE 1a for knee pain • 40% have stinging, burning, erythema