Download
1 / 25
250 likes | 268 Views
Learn about the practicality and flexibility of Hemodialysis in critically ill patients, comparing different modalities and outcomes. Discover tips, limitations, and considerations for efficient hemodialysis treatment.

E N D
Practicality and Flexibility of Application • IRRT also allows more liberty for patient care and investigations outside the treatment and monitoring unit, by offering a dialysis-free period, without loss of dialysis time or adequacy • IRRT machines can be used in an extended protracted mode when needed, and the treatment time can be decreased coupled to an increase in efficacy when the condition of the patient improves • CRRT machines, do not allow an increase of the intensity of the treatment to allow shorter treatments Crit Care 2010, 14:R46
What to Choose? PD is available 100% in developing and developed country Raina et al. PLoS ONE 12(5): e0178233.
Modality of Choices Raina et al. PLoS ONE 12(5): e0178233.
Limitation of Expenses Median difference was US$289.6 per day in disfavor of CRRT ;The main differences attributed to fluid replacement and the extracorporeal circuit; reducing the substitution volume to <25 ml/minute/kg, diminished cost only by US$67.2 per day
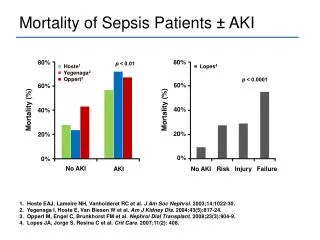
Pediatric Acute Renal failure: Outcome by Modality and Disease • Low BP at onset of RRT (33% vs 61% with nl BP, vs 100% with high BP; P<0.05) • Use of pressors anytime during RRT ( survival 35% vs 89; P<0.01) • Diagnosis (primary renal failure with a high likelihood of survival vs secondary renal failure) • RRT modality (40% survival with HF, vs 49% survival with PD, vs 81% survival with HD) • Pressor use was significantly higher in children on HF (74%) vs HD (33%) or PD (81%) Ped Neph 2001, Volume 16,iss 12; pp 1067-71
Caveats to CRRT No evidence from randomized trials to support survival advantage Risk of complications related to anticoagulation is higher Training and equipment costs
Comparison of Solute Clearance in three modes of CRRT • CVVHD was superior to predilution CVVH for CL of urea and Cr • Qb~ 60 mL/min • While predilution or dialysate was run at 16.7% :33% :50% Qb • CVVHD had a superior clearance • 15% greater clearance at 1200 and 1800 mL/hr (P<0.05) and 10% at 600ml/hr PCCM: May 2004, Volume 5, Issue 3 – pp 269-274
Solute Removal: Is convective Mode is better Than Diffusive Clearances? • CRRT promotes solute removal due to better mobilization from extra-plasmatic compartments • More down time with CRRT vs IRRT due to filter exchange • ? But higher intensity of solute removal leads to greater removal of drugs resulting in inadequate drug concentrations (for example, of antimicrobials) or more electrolyte disturbances • Removal of cytokines and other large molecules can be obtained just as well, if not better, with IRRT or SLEDD, with large pore size (so-called high-flux membranes) • No survival advantage of more efficient removal over standard removal. Intensive Care Med 1997, 23:288-296 and Crit Care Med 2010, 38:1360-1369
Hemodynamic Stability and Fluid Removal • If there is a hemodynamic benefit for CRRT, this nevertheless is not translated into differences of survival • Clinical hemodynamic parameter that was significantly higher with CRRT than with IRRT; the number of hypotension episodes was not different. • However, potentially blurring the results of RCTs comparing CRRT and IRRT is the reluctance for including patients with major hemodynamic problems
Blood volume continuous monitoring (BVM) : refilling capacity test, secured and optimized UF Blood thermal monitoring (BTM) : vascular stability, regional blood flow potential impact HDF procedure : allowed sequential UF, HF, HD, adapted to the individual patient needs, and evolution; on-line HDF provide for the restitution- hemofiltration fluid (possibility for adapted sodium concentration) Profiled prescriptions: UFrate at the best intermittent (refilling time), NaD not too high (interstitial storage, edema) Clearance and dialysis dose measurement, dialysis efficiency: slow (urea osmotic tolerance) but controlled purification (potassium gradient) Power Tools for Acute Hemodialysis not Too TrickyvTricks……..I am not dealing with old Hemodialysis Machine
Pediatric Intradialytic Hypotension: A Systematic Review • N=148 (2 days – 18yr), (3.2 to 61.4 kg) • Incidence of IDH ranged (19.6% - 75%) with lower percentages who received NIVM during HD (implemented 65%) • Of the protective maneuver tested Linear NaM, HNA, NIVM and low temp 35.5-35 were effective in reducing IDH but NIVM was favored by some plurality • Sequential UF was not effective in reducing IDH Raina et al. Poster presentation pCRRT
Most important factor: effluent volume (determined by flow rate and therapy duration)1 Effluent rates have significantly increased compared to prior recommendation, eg “Drug Prescribing in Renal Failure”, 2007 ed. Assumes CRRT effluent rate of only 2 L/H2 Calculated CRRT dosing charts may be Outdated due to increased flow rates and efficiency of newer dialyzers3 Variability in published recommendations potential underdosing in CRRT Drug Clearance by CRRT • Mueller BA, et al. Organs 2003 • Aronoff GR, et al. Drug prescribing in renal failures: dosing guidelines,2007, ACP • Heintz BH, et al. 2009, Pharmacotherapy
Restriction of Bleeding Complications • CRRT Citrate option depends on skilled personnel and any mistake or technical problem may have grave consequences, such as life-threatening hypocalcemia- Crit Care Med 2009, 37:545-552 • Bleeding complications were more frequent in the CRRT group and were the major reason for switching modalities from CRRT to IRRT- Curr Opin Nephrol Hypertens 1999, 8:701-707 • Filter clotting tends to occur more frequently with CRRT than with IRRT 51% vs 22% (p<0.001)- Int. J Artif Organs 2004:;27(5):371-9 • IRRT had less need for anticoagulation, and patients could be treated without coagulation at all
Dialysis Circuit Heparin Pump Blood Pump Arterial Pressure Monitor Dialysate Pump Dialysis Access Venous Pressure Monitor Air Trap Femoral Vein Ultrafiltrate Dialysate
Blood Priming • If the extracorporeal volume (tubing volume + dialyzer volume) exceeds 10% of the patient’s estimated blood volume (> 80 ml/kg), consider priming the circuit with blood to prevent instability when initiating hemodialysis) • This usually applies to children weighing less than 10 kg
Blood Priming • Diluted PRBC (hematocrit 35%) that has been typed and cross-matched with the patient. • Prime the circuit per routine, using normal saline • Inject 2 units of heparin per ml into the diluted PRBCs. • Prime the dialysis circuit with the diluted PRBCs. • Allow the system to recirculate for 5 minutes to heparinization it and to warm the blood to an appropriate level for the patient. • In any child in whom a blood prime is used, give the entire blood prime by connecting the arterial and venous lines simultaneously • In patients 10-15 kg or hemodynamically unstable patients, give half or all of the prime • In patients > 15 kg who are hemodynamically stable, do not give the prime.
Patient monitoring/Management of Hypotension • Vital signs q 30 minutes • Crit-line monitoring and/or Linear NaM and Cooling of dialysate increase vascular tone and support BP. • Prior to initiating dialysis, orders should be in place for treatment of hypotension unresponsive to adjustment in UF goal per Crit-line. • Saline bolus: 5 ml/kg • 25% albumin 0.25 gm/kg, maximum 12.5 gm • Mannitol 0.25 gm/kg, maximum 12.5 gm. • no more frequently than q 1 hr. • Not he last hour of treatment. • Vasopressor support to correct dialysis-associated hypotension.
HD Prescription The staff member performing dialysis must remain within visual and auditory range of the patient/dialysis machine In patients without a blood prime, return the blood in the system per routine In children <20 kg, slow the blood flow rate by 50% while returning the blood to prevent acute hypertension In patients in whom a blood prime is used, do NOT return the blood in the system to the patient. Discard the entire setup with the blood in it to avoid acutely increasing the child's blood volume.
Modality: No overall benefit to CRRT compared to IHD, though CRRT may be better for patients at risk of increased ICP and for volume control Dose: No benefit to “intensive” therapy, but delivered dose of both CRRT and IHD must be monitored to ensure minimum adequate dose Anticoagulation: Citrate is gaining wider acceptance as the preferred anticoagulation for CRRT Buffer: Bicarbonate should be the buffer in dialysate and replacement fluid for RRT in patients with AKI, especially with liver failure and/or lactic acidemia Summary