Download
1 / 18
180 likes | 422 Views
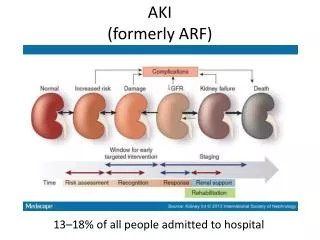
AKI. Sarah Edwards – ST5 renal. Objectives. Be able to recognise acute kidney injury Understand risk factors for developing AKI Form a simple differential diagnosis for cause of AKI Select appropriate investigations Know how to treat hyperkalaemia and initiate management of AKI. Scenario.

E N D
AKI Sarah Edwards – ST5 renal
Objectives • Be able to recognise acute kidney injury • Understand risk factors for developing AKI • Form a simple differential diagnosis for cause of AKI • Select appropriate investigations • Know how to treat hyperkalaemia and initiate management of AKI
Scenario • 73 year old man presents to A&E with 48 hr diarrhoea and vomiting. Can’t remember passing urine today. • He’s been waiting for a while to be seen, a nurse hands you some blood results that the lab have phoned through; Na 135 K 6.7 Ur 20 Creat 258
He’s got an AKI Think of Simple Differential Diagnosis Is this? • Pre-renal • Renal • Post-renal Or mixture?
History • He has a PMH of hypertension. • He takes atenolol and ramipril • Non smoker, no alcohol
Examination • BP 100/65 HR 64 RR 20 SpO2 97% RA • Dry mucous membranes • No oedema • Chest clear, Abdo soft non tender, HS normal
What next? Life saving things first…
Treat the potassium Principles of treating Hyperkalaemia • Cardiac stabilisation = calcium gluconate • K redistribution therapy = insulin/ dextrose • Ensure excretion, i.e patient is passing urine • Others calcium resonium, dialysis
Investigations • Urinalysis and MSU • US KUB • Renal bloods screen • ANCA, ANA, DsDNA, antiGBM, C3C4, • Myeloma screen sFLC, SPE • Renal referral ? Biopsy if intrinsic renal cause suspected
Management • Treat hyperkalaemia • Fluid management – catheter, fluid balance IV fluids and repeated examination • Medication review – stop nephrotoxins, caution renal excreted drugs • Look for and treat cause
Management • Pre-renal – fluids and address cause • Renal – renal team • Post-renal – urinary catheter, if obstruction above the bladder needs nephrostomy
When do we dialyse? Depends on the complications of AKI…
Complications of AKI • Hyperkalaemia • Pulmonary oedema • Metabolic acidosis
Key points • AKI is common, particularly if pre-existing CKD, elderly, diabetic, heart failure,taking nephrotoxic medication • Work through potential pre-renal, renal and post-renal causes • Examination, urinalysis and USS are key • Insulin/dextrose is only a temporary treatment measure for hyperkalaemia