Download
1 / 36
360 likes | 466 Views
Addressing ADHD in HBFT. Nancy O’Conner, MS, LCMFT C.R. Macchi, PhD, LCMFT Home-based Family Therapy Partnership The Family Center Kansas State University HBFTPartnership.com. Learning Objectives. Participants will… Part I

E N D
Addressing ADHD in HBFT Nancy O’Conner, MS, LCMFT C.R. Macchi, PhD, LCMFT Home-based Family Therapy Partnership The Family Center Kansas State University HBFTPartnership.com
Learning Objectives Participants will… Part I • Identify the child and other family member experiences of Attention-Deficit Hyperactivity Disorder (ADHD) • Review the context of ADHD along the continuum of behavior disorders • Review the diagnostic criteria of ADHD and the varying presentations of the diagnosis • Identify common co-morbidities associated with ADHD • Develop greater awareness of the controversies associated with the diagnosis of ADHD Part II (March 27th) • Explore effective individual and family-focused treatments for ADHD • Understand the suspected and known treatment side-effects • Review ways to collaborate with medical and school officials to help families manage the effects of ADHD
The Experience of ADHDNoelle Demo’s Story Public Broadcasting Service. (2001). Medicating kids. In S. Audette (Ed.), Frontline and Rain Media, Inc.
Historical Development of ADHD Diagnosis • BRAIN DYSFUNCTION (1900s to 1960s) • Defective moral control of behavior • Brain damage syndrome • Minimal brain dysfunction (MBD) • Inclusion of inattention and impulsive behavior • BEHAVIORAL SYNDROME (1950s to 1970s) • Hyperactivity/hyperkenesis • ATTENTION DEFICIT DISORDER (1980s to present) • Attention deficit • Behavioral inhibition • MOTIVATIONAL DEFICIT DISORDER (1990s to present) • Insensitivity to behavioral consequences Barkley, R. (2006). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (3rd ed.). New York: Guilford.
Etiology of ADHD • Neurological factors • Brain composition and functioning • Neurochemical imbalance • Genetic factors • Psychosocial ecological • Technological developments • Enculturation • Child rearing • Environmental factors • Toxins • Diet • Nutrition
Hyperactivity Poor filtering and lower threshold of stimulation
Attention-Deficit Diminished brain activity in the brain’s behavioral inhibition system (BIS) resulting in decreases of self-regulation and executive functioning
Motivational Deficit Neurological conditions produce an insensitivity to consequences
Motivational Deficit Framework Consequence/Reinforcement
ADHD Prevalence Rates • An estimated 3%-7% of children suffer from ADHD • Some studies suggest higher rates in community samples • 4:1 ratio of boys to girls with ADHD • Diagnosed approximately three times more often in boys than girls • 30-50% of those diagnosed with Predominantly Inattentive type of ADHD have what is known as “sluggish cognitive tempo” (SCT) • Approximately 44% can be diagnosed with an additional psychiatric disorder (comorbidity) • Approximately 35% of children have major depression • 40% of children and 65% of adolescents with ADHD also meet criteria for ODD American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th, text revision ed.). Washington, D.C.: American Psychiatric Association.
ADHD Statistics • 50% have problems in relationships with others • There is a 25-35% probability that if one person in a family is diagnosed with ADHD, another person within the family has it as well • Research indicates that children with ADHD are significantly more likely to be injured (injured while riding bicycle, head injury, injure multiple parts of the body, and accidental poisoning) than those without the diagnosis • Children with ADHD seem to have significantly higher medical costs Barkley, R. (2006). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (3rd ed.). New York: Guilford.
Continuum of Diagnoses Pervasive Adult Disorder Childhood Disruptive Behavior Normal Behavior & Adjustment ADHD Oppositional Defiant Disorder Conduct Disorder Antisocial Personality Disorder • Task-focused • Delayed gratification • Compassionate • Cooperative • Personal responsibility • Hyperactivity • Inattention • Impulsivity • Defiance • Anger • Blaming • Aggression/Cruelty • Destruction • Theft • Egosyntonic/Enduring • Aggression/Cruelty • Destruction • Theft
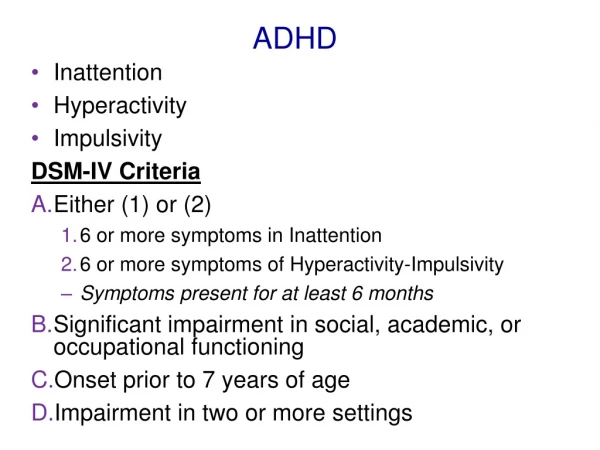
Types of ADHD • Inattentive Type • Hyperactive-Impulsive Type • Combined Type American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th, text revision ed.). Washington, D.C.: American Psychiatric Association.
General Criteria for All Types of ADHD • Symptom occurrence • Persisted for 6 months or longer • Maladaptive and inconsistent with developmental level • Some of the symptoms that caused the impairment were present before 7 years old • Some impairment is present in two or more settings • Clear evidence of clinically significant impairment in social, academic or occupational functioning • Types of the symptoms which often apply (six or more) • Each criteria is prefaced with the word “often” underscoring the unusual frequency of the presenting symptoms
Criteria for ADHDSymptoms of Inattention • Fails to give close attention to details • Makes careless mistakes in schoolwork, work, or other activities • Difficulty sustaining attention in tasks or play activities • Does not seem to listen when spoken to directly • Does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions) • Difficulty organizing tasks and activities • Avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (such as schoolwork or homework) • Loses things necessary for tasks or activities (e.g., toys, school assignments, pencils, books, or tools) • Easily distracted by extraneous stimuli • Forgetful in daily activities
Clinical Examples ofInattention • What are the variety of presentations you have noticed in a child who has attention difficulties? • What are the implications of using a motivational deficit framework for understanding the child’s inattention?
Criteria for ADHDSymptoms of Hyperactivity-Impulsivity • Hyperactivity • Fidgets with hands or feet or squirms in seat • Inappropriately leaves seat in classroom or in other situations • Inappropriately runs or climbs (in adolescents and adults, may be limited to subjective feelings of restlessness) • Difficulty playing or engaging quietly in leisure activities • “On the go” or often acts as if “driven by a motor” • Talks excessively • Impulsivity • Blurts out answers before questions have been completed • Difficulty awaiting turn • Interrupts or intrudes on others (e.g., butts into conversations or games)
Clinical Examples ofHyperactivity-Impulsivity • What are the variety of presentations you have noticed in a child who has hyperactivity-impulsivity issues? • What are the implications of using a motivational deficit framework for understanding the child’s hyperactivity-impulsivity issues?
Behavioral and Social Features of ADHD • Low frustration tolerance • Rejection by peers • Poor self-esteem • Academic achievement impaired • Family relationships often characterized by resentment and antagonism
Differential Diagnoses • Age-appropriate behaviors • Anxiety Disorders – PTSD, Generalized Anxiety Disorder • Environments • Understimulating (i.e. classroom) • Disorganized, chaotic • Learning disorders • Medication reactions effecting behaviors (e.g., bronchodilator for asthma) • History of trauma • Bipolar Disorder • Schizophrenia
Other Conditions that Mimic ADHD • Hypoglycemia • Allergies • Learning disabilities • Hyper or Hypothyroidism • Hearing and vision problems • Early onset diabetes • Heart diseaseand other cardiac conditions • Early onset Bi-Polar disorder • Exposure to some toxins
Other Conditions that Mimic ADHD • CAPD (Central Auditory processing Disorder) • Worms • Viral or bacterial infections • Malnutrition or improper diet • Head injuries • Streptococcus • FAS or FAE • Trauma
Co-morbidity of Disorders • Higher prevalence of the following • Mood Disorders • Anxiety Disorders • Learning Disorders • Oppositional Defiant Disorder • Conduct Disorder • Substance-related Disorders
ADHD Assessment • Interviewing the child • Interviewing the parents • Parent observations of the child’s experiences with ADHD • Assess for ADHD in the parent(s) • Providing a teacher assessment of child classroom behaviors and peer relationships
Behavioral Severity Scales Warren, M. (2002). Behavioral management guide: Essential treatment strategies for the psychotherapy of children, their parents, and families. Northvale, NJ: Jason Aronson.
Motivational Deficit Framework Consequence/Reinforcement
Motivational Assessment • Determine the child’s… • Level of sensitivity to external stimuli • Degree of internal locus of control • Level of perceived responsibility for behaviors • Level of responsiveness to behavioral reinforcements • Emotional connection to parents
Motivational Assessment • Determine the parents’… • Maintenance of environmental stability • Types and uses of natural consequences • Level of responsiveness to child’s needs • Attempts to reinforce child’s internal locus of control • Emotional connection to the child • Interpretations of child behaviors
Discuss Implications of Motivational Focus • Assessment • Treatment planning • Interventions ** Email facilitators with specific clinical presentations. We will integrate our discussion of treatment planning and interventions to address those specific issues during Part II.
Controversies Over ADHD Diagnosis • Neurological factors • Medical factors • Behavioral factors • Social factors
Part II – Treatment and Interventions of ADHD • March 27th, 9:00am-Noon • Learning objectives – Participants will… • Explore effective individual and family-focused treatments for ADHD • Understand the suspected and known treatment side-effects • Review ways to collaborate with medical and school officials to help families manage the effects of ADHD