Download
1 / 22
220 likes | 406 Views
Pain ,opiate analgesics and antagonists -02. Dr. Israa. II. Other Opioid (Narcotic) Analgesics. A. Heroin ( diacetyl morphine) μ - agonist Heroin is more lipid soluble than morphine and about 2½ times more potent It enters the CNS more readily

E N D
II. Other Opioid (Narcotic) Analgesics A. Heroin (diacetyl morphine) • μ- agonist • Heroin is more lipid soluble than morphine and about 2½ times more potent • It enters the CNS more readily • It is a schedule I drug and is not used clinically, but it is a drug of abuse.
B. Codeine • From opium or synthesized by methylation of morphine • Has a much better oral /parenteral absorption ratio than morphine. • Effective for mild to moderate pain, cough, diarrhea. • Metabolized in part to morphine by O-demethylation. • μ- receptor agonist. • Has a more potent histamine-releasing action than morphine. • Dependence liability of codeine is less than that of morphine, . • It is 1/12 as potent as morphine
C. Dextromethorphan: • Excellent oral antitussive • No analgesic effect • No GI effects • No respiratory depression
D. Meperidine (Pethidine) • Produces analgesia, sedation, euphoria and respiratory depression. • Less potent than morphine, 80-100 mg meperidine equals 10 mg morphine. • Shorter duration of action than morphine (2-4 hrs). • Meperidine has greater excitatory activity than does morphine and toxicity may lead to convulsions. • Meperidine appears to have weak atropine-like activity. • It does not constrict the pupils to the same extent as morphine.
Does not cause as much constipation as morphine • Purely synthetic μ- agonist • Not an effective antitussive agent. • less effect in uterine contraction commonly employed in obstetrics also causes less urine retention Adverse reactions : • Respiratory depression • Tremors • Delirium(illusion-error,disorientation,hallucination,& extreme excitement) and possible convulsions • Dry mouth • Severe reaction if given with MAOI, consists of excitement, hyperthermia and convulsions; it is due to accumulation of pethidine(norpethidine) metabolite but the details are still unclear.
E. Fentanyl • μ- agonist, related chemically to meperidine. • Approximately 80 times more potent than morphine, main use in anesthesia . • Duration of action very short (t1/2 = 20 min). • Can be given IM, IV, transdemally or via patient controlled infusion system may be given intrathecally • Often used during cardiac surgery because of its negligible effect on the myocardial contractility
F. Sufentanil • A synthetic opioid related to fentanyl. • About 7 times more potent than fentanyl. • Has a slightly more rapid onset of action than fentanyl.
G. Methadone • Pharmacology and analgesic potency similar to morphine; μ- receptor agonist. • Very effective following oral administration. • Longer duration of action than morphine due to plasma protein binding (t1/2 approximately 25 hrs). • Used in methadone maintenance programs for treatment of opioid addicts and for opiate withdrawal syndrome(it reduces the physical abstinence syndrome)make it possible to wean the addict from opioids.
H. Propoxyphene • A methadone analog. • Used orally to relieve mild to moderate pain, it is weak analgesic ;often combined with Paracetamol . • Has a low addiction potential • The most common adverse effects are: dizziness, drowsiness, and nausea and vomiting. • CNS depression is additive with other CNS depressants (alcohol and sedatives). • can cause cardio- toxicity and pulmonary edema which can not reversed by naloxone
III. Mixed Narcotic Agonists/Antagonists • These drugs produce analgesia, but have a lower potential for abuse and do not produce as much respiratory depression.
A. Pentazocine • қ- agonist (analgesia) and μ-antagonist (less respiratory depression). • Orally, it has about the same analgesic potency as codeine. • Adverse reactions: Nausea, vomiting, dizziness, dysphoria, nightmares and visual hallucinations. • Rarely used nowadays
B. Nalbuphine • Resembles pentazocine pharmacologically. • Like morphine, nalbuphine reduces myocardial oxygen demand. May be of value following acute myocardial infarction due to both its analgesic properties and reduced myocardial oxygen demand. • Most frequent side effect is sedation. • Less propensity to produce psychotomimetic side effects
C. Butorphanol • Resembles pentazocine pharmacologically. • 3.5 to 7 times more potent than morphine. • Not available for oral administration • They exhibit ceiling of respiratory depression effect
D. Buprenorphine • A partial agonist at μ-receptor. • 200 times more potent than morphine. • Low potential abuse, but can precipitate withdrawal in addicts • In naive persons it acts like morphine • Major use is office-based detoxification of opioids • Causes less sedation, respiratory depression and hypotension even in high doses.
IV. Opiate Antagonists Opiate antagonists have no agonist properties. They are utilized to reverse opiate induced respiratory depression and to prevent drug abuse. A. Naloxone (Narcan) • Pure opiate antagonist at all opioid receptors • Given parenterally -Short duration of action (1-4 h) • Can precipitate withdrawal in addicts.
B. Naltrexone • Oral pure opioid antagonist • Long duration of action • Contraindicated in liver disease • Used in late stages of opioid addiction treatment ( also in treatment of alcoholism). C. Nalmephine • Long-acting parenteral opioid antagonist.
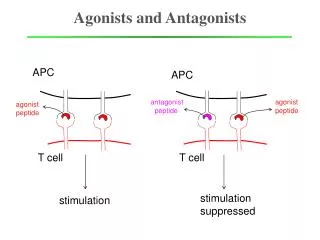
Antitussives Chemical & mechanical Afferents EFFerents Stimuli Respiratory muscles Sensory receptors in upper respiratory tract Cough Center medulla
Antitussives • Antitussives: against cough • Coughing is a protective reflex • Antitussives depress cough center, therefore depress the cough reflex. • Antitussives should not be used in productive cough.
Antitussives include: 1. Opioids: • Codeine, dextromethorphan, hydrocodone, hydromorphone. • They are opioid agonists against dry cough. • They are of low abuse potential. • Side effects: drowsiness and constipatiopn.
2. Non-opioids: • E.g. butamirate citrate which depress the cough center. 3. Peripherally acting antitussives: • These prevent irritation of sensory receptors in the upper respiratory tract. 4. Local anesthetics • also depress the cough center. They include: • demulcents: liquorice, honey • local anesthetics: benzonatate
THANK YOU • REFRENCES: • RANG AND DALE • LIPPINCOTTOS • LANGE • TABLES FROM DR.KUKAB SLIDES