Download
1 / 102
1.85k likes | 5.85k Views
MANAGEMENT OF DEEP CARIES LESIONS. INTODUCTION HISTORY INFECTED & AFFECTED DENTIN EFFECT OF CARIES ON P-D ORGAN DIAGNOSIS OF DEEP CARIES LESION INDIRECT PULP CAPPING DIRECT PULP CAPPING.

E N D
INTODUCTION • HISTORY • INFECTED & AFFECTED DENTIN • EFFECT OF CARIES ON P-D ORGAN • DIAGNOSIS OF DEEP CARIES LESION • INDIRECT PULP CAPPING • DIRECT PULP CAPPING
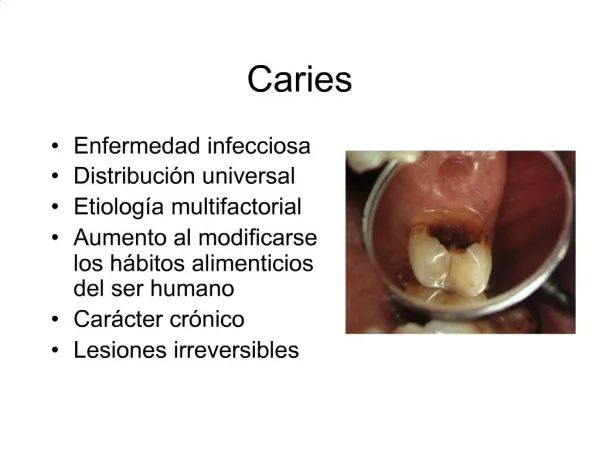
Deep carious lesions are those in which caries penetration is easily observed in the dentin and may involve more than one half of the dentin thickness between the DEJ and the pulp. INTRODUCTION
HISTORY • 1756- Phillip Pfaff used gold leaf over exposed vital pulp to promote healing. • 1826- Leonard Kocher published principles of dental surgery.. • 1867- Atkinson highlighted the use of creosote for the treatment of dental pulp. • 1915- G.V. Black reported dissatisfaction with technique of pulp capping..
1930- Herman advocated use of calcium hydroxide for pulp capping. • 1940- Orbans research led to realization that the dental pulp possess definite powers of recuperation and repair. • 1938- Teuscher & Zander reported action of calcium hydroxide and also described formation of dentin layer called “dentin bridge”. • 1964- Pisanti & Sciaky and stark et al used radio active calcium to identify source calcium in dentin bridge • 1992- Rebel quoted that “exposed pulp is a doomed organ”.
ZONES OF DENTINAL CARIES • Any dentinal carious lesions in vital P-D organ will exhibit five layers or zones under optical microscope. Decayed zone Septic zone Decalcification of dentin Opaque zone Transparent zone
Completely devoid of minerals Complete decomposition of organic matrix Collagen fibers.. High concentration Of microrganisms and plaque deposits DECAYED ZONE
Mineral crystals.. Dentinal tubules.. Collagen fibers. Highest conc. Of microorganisms SEPTIC ZONE
Clinically it is the most significant zone,both diagnostically and therapeutically. Mineral crystals.. Dentinal tubules.. Collagen fibers.. Repair activities.. DEMINERALIZED ZONE
Area of undisturbed mineralization repair Zone of dentinal slerosis.. Clinically.. TRANPARENT ZONE
Found pulpal to the transparent zone. Characterized by intratubular fatty degeneration. OPAQUE ZONE
EFFECTS OF CARIES ON P-D ORGAN. • Carious process has three distinct forms of irritants 1. Biologic irritants 2. Chemical irritants 3.Physicomechanical irritants.
Type of decay. • Duration of decay. • Number and pathogenecity of micro organisms. • Tooth resistance
Individual reaction of the P-D organ Tooth age, Patients age, Cellularity & vascularity of the pulp and root canal system .
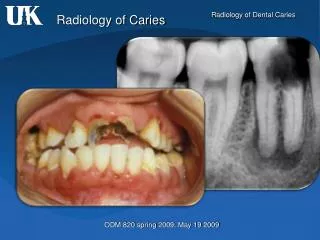
DIAGNOSIS OF DEEP CARIES LESIONS 1.Pain. 2.Radiographs. 3.Pulp testing. 4.Percussion Tests. 5.Visual examination and tactile examination. 6.Selective Infiltration or ligamental anesthesia. 7.Use of dyes. 8.Test cavity preparation.
PAIN • Serves guiding criteria,but cannot be solely used as diagnostic criterion. • pain threshold • Non vital teeth-frequently painless • Spontaneous pain… • Pain on stimulus..
proximity of the carious lesion to the pulp chamber and root canal system Effective depth. The area of minimum thickness of sound dentin separating the pulpal tissue from the carious lesion. RADIOGRAPHS
Vital capacity of p-d organ • Pulp changes.. • Location of the caries cone tip relative to the anatomy of the pulp chamber and root canal system. • Thickness of the periodontal ligament space and intactness of lamina-dura
Relative size of the apical foramen to that of the pulp chamber and root canal system. • Dimension of a pulp exposure relative to the dimensions of the pulp chamber and root canal system. • Gross evaluation of mineralization, presence of sclerotic dentin and calcific barrier.
PULP TESTING • It includes Thermal test heat test cold test Electrical pulp testing
It can be performed with Compound Guttapercha sticks Hot burnisher Rubber cup/wheel warm water in a syringe Preffered temp. is 65.50c HEAT TEST
It can be perfomed with cotton pellet soaked with Ethyl chloride, Sticks of ice, Carbon dioxide snow, Refrigerant spray. COLD TEST.
RESPONSE TO THERMAL TEST • Normal reponse • Abnormal response • No response Non vital teeth Vital teeth with false negative response
It is performed with instruments battery or alternating current powered electrodes. When a positive response is obtained, comparisons should be made with the adjacent, opposing and contra-lateral teeth. Electrical Pulp Test
Minimum energy needed to illicit a response is noted in control teeth • Required energy is higher in the control teeth, this is an indication of possible acute changes in the P-D organ of the affected tooth. • Lower in the control teeth, this may indicate possible progressive chronic changes, advance repair
Reasons for false positive response: Electrode contacts the gingival tissue. Anxious patient. In case of liquefaction necrosis. Failure to isolate and dry the teeth properly. Multi rooted teeth.
Reasons for false negative response- Patients who are premedicated Inadequate contact of electrode with the tooth structure. Recently traumatized tooth. Recently erupted teeth with an immature apex. Partial pulp necrosis or calcification in the canal.
Determine whether the inflammatory process has extended into the periapical tissues Quite unreliable. PERCUSSION SENSITIVITY
VISUAL AND TACTILE EVALUATION OF DENTIN • The use of explorer gives an idea of type of dentin in preparation walls and floors • Presence of sclerotic dentin indicates.. • Presence of grayish pink or grayish brown..
SELECTIVE INFILTRATION OR LIGAMENTAL ANESTHESIA. • If the pulpal symptoms described by patient involves a total side or a quadrant, local or periodontal infiltration anesthesia for most suspected teeth stops the pain.
0.5% Basic fuchsin in propylene glycol is used. Fuchsin is applied to the dentin for 10 second. The nature of the collagen fibers constitute the difference in the stainability of the two layers of dentin. DYES TO DIFFERENTIATE BETWEEN REPARABLE AND IRREPARABLE DENTIN
N- NORMAL DENTIN 1- INFECTED DENTIN 2- AFFECTED DENTIN
TEST CAVITY • Made by drilling through the enamel dentin junction of an unanesthetized tooth. • Drilling should be done at slow speed. • Sensitivity or pain felt by the patient is an indication of vital pulp.
DIRECT PULP EXPOSURE • Pin- point exposure having sound dentin at the periphery of the exposure with no hemorrhage in a vital P-D organ is an indication of either no pulpal inflammation or a mild degree of pulpal inflammation. • Exposure having decayed or infected carious dentin at its periphery would indicate considerable inflammation beyond exposure site. The reparability of this type of exposure is doubtful
Exposure accompanied by profuse hemorrhage could be an indication of great involvement of the pulpal and root canal tissues. • Exposure accompanied by inflammatory fluids or pus is evidence of extensive inflammation and destruction of the pulpal and root canal tissues.
Exposure is very close to anatomical constrictions in the pulp chamber or root canals, the chances of repair is very less. • Lower the ratio of exposure to dimensions of pulpal and root canal tissues greater the possibility of repair.
INDIRECT PULP CAPPING • DEFINITION • HISTORICAL REVIEW • OBJECTIVE • RATIONALE • INDICATIONS • CONTRAINDICATION • TECHNIQUES
Defined as incomplete excavation leaving a thin layer of residual carious dentin (King et al. 1965) Defined as the application of a medicament over a thin layer of remaining carious dentin, after deep excavation, with no exposure of the Pulp . DEFINITION
OBJECTIVE • To avoid pulp exposure… • To maintain pulp vitality by 1. Arresting carious process 2. Promoting dentinal sclerosis 3. Stimulating formation of tertiary dentin. 4. Remineralizing caries lesion
RATIONALE • Active dentinal caries has three layers 1. Outer soft necrotic layer.. 2. A firm discolored dentin.. 3. A hard discolored deep dentinal layer.. • The basic principle is..
HISTORICAL REVIEW • The concept of indirect pulp capping was first described by Pierre Fauchard as reported by John Tomes in the mid-18th century. • In 19th century John Tomes stated that, “it is better that a layer of discolored dentin should be allowed to remain for the protection of the pulp rather than the risk of sacrificing the tooth”.
1891- W.D Miller discussed various “antiseptic” that should be used for sterilizing dentin. • In contast G. V. Black stated that, “no decayed or softened material should be left in a cavity preparation, whether or not the pulp was exposed”.
INDICATIONS 1. History a. Mild discomfort from chemical/thermal stimuli b. Absence of spontaneous pain. 2. Clinical examination a. Large carious lesion b. Absence of lymphadenopathy c. Normal appearance of adjacent gingiva. d. Normal color of the tooth.
3. Radiographic examination a. Large carious lesion in close proximity to the pulp b. Normal lamina dura c. Normal periodontal ligamental space d. No interradicular or periapical radiolucency
CONTRAINDICATIONS 1.History a. Sharp, penetrating pain that persists after withdrawing stimulus b. Prolonged spontaneous pain, particularly at night. 2.Clinical examination a. Excessive tooth mobility b. Tooth discoloration c. Nonresponsiveness to pulp testing techniques
3.Radiographic examination a. Large carious lesion with apparent pulp exposure b. Interrupted or broken lamina dura c. Widened periodontal ligament space d. Radiolucency at the root apices or furcation areas.