Download
1 / 29
300 likes | 329 Views
Ruptured Infected Femoral Artery Pseudoaneurysms in IV Drug Addicts. Winston Wong, Yan Chai Hospital JHSGR July 18 2015. Next 10 minutes…. Background Management Controversies. Background. IV drug abuse is an increasing problem with concomitant increase in its complications

E N D
Ruptured Infected Femoral Artery Pseudoaneurysms in IV Drug Addicts Winston Wong, Yan Chai Hospital JHSGR July 18 2015
Next 10 minutes… • Background • Management • Controversies
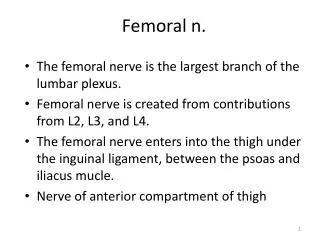
Background • IV drug abuse is an increasing problem with concomitant increase in its complications • Vascular complications from IV drug abuse is on the rise • Infectious pseudoaneurysms • Deep vein thrombosis • Venous gangrene • Arterial embolization • Infected pseudoaneurysms of the femoral artery are one of the most common arterial complications in IV drug abusers
Pathophysiology • Repeated non-sterile punctures aimed at finding easy peripheral venous access • Extravasation of blood • Contamination of the subsequent hematoma • Erosion and eventual rupture of the vessel wall • Formation of infected pseudoaneurysm
Potential complications • Distal embolization • Limb loss • Sepsis • Rupture with rapid blood loss • Death
Presentation • Groin injection site • Groin mass • Drainage / bleeding • Pulsatility • Thrill • Absent pedal pulses • Inability to extend hip • Septicemia
Overview • Background • Management • Controversies
Broad spectrum IV antibiotics Universal contact precaution Adopted from Tan et al, World J Surg. 2009
Bacteriology? • Pre-antibiotic era: Enterococcus, streptococcus [1] • Post-antibiotic era: Staph aureus, Salmonella [1] • Ting & Cheng (HK)[2] MSSA • Jayaramans (US)[3], Saini (India)[4]Staph aureus (majority), Pseudomonas, E coli • Brossier et al (France)[5] Majority from atypical bacteria e.g. Campylobacter, Listeria, MTB, CoxiellaStaph aureus (4%)
Principles of surgery • Stop bleeding • Debride infective tissue • Preserve distal circulation • Conservative management is rarely an option
Overview • Background • Management • Controversies
Proposed treatments? [6] • Ligation & excision (Lig-Exc) alone • Lig-Exc + immediate revascularization • Lig-Exc + delayed revascularization + Debridement of infective tissue
Ligation & excision • Single vs triple ligation (CFA, SFA, PFA) • Benefits • Faster, more straightforward • Require less resources & expertise • Complications • Claudication (~40-50%, some studies up to 100% [7]) • Amputation (none to 35.0% [6])
Ligation & excision • Cheng et al, 1992 [8] • 21 infected femoral pseudoaneurysms • 19 ligations only, 2 with revascularization • 14 reported claudication (74% of ligation only) • Ting & Cheng, 1997 [2] • 33 infected femoral pseudoaneurysms • 24 triple ligation, 10 single ligation • 4 asymptomatic and rest had some degree of claudication • No limb loss in both studies
Considerations in revascularization? • Revascularization is challenging and often require special technical considerations • Autogenous vs synthetic grafts? • Autogenous veins are more resistant to infection, but not always available [6] • Arterial grafts (e.g. internal iliac artery) [9] • Synthetic grafts [6,10] • Significantly higher risk of reinfection • Life-threatening hemorrhage if used as route for injections
Considerations in revascularization? • Extra-anatomic vs in-situ bypass? • In-situ bypass through infected field is controversial • Extra-anatomic via lateral thigh or obturator route • High chance of graft failure requiring removal • Immediate vs delayed revascularization? • Close observation for signs of limb ischemia • Worse outcome if delay in revascularization > 6 hrs [11] • Contraindications? • Presence of extensive tissue necrosis • Necrotizing fasciitis
Endovascular surgery? • Emerging interest as scattered reports of successful repair of infected aneurysms in several territories • Minimally invasive alternative / bridge to open surgery • Prosthesis in infected field is always debatable
Endovascular surgery? • Handful of case reports only for endovascular intervention for ruptured femoral infected pseudoaneurysms [15, 16] • ? Prolonged / lifelong suppressive antibiotic regimen • 6 weeks? 6 months? Lifelong? • ? Antiplatelets / anticoagulation • ? Long-term consequences • ? Patient selection
In the middle of the night… • Resuscitation • Surgery • Hemostasis - ligate involved arteries • Infection control - excise pseudoaneurysm, debride tissue • Bacteriology – save pus / wall for cultures • Wound – leave open / partial close for dressing • Beware of needle prick! • Post-op • +/- Revascularization
Conclusion • The best surgical management of infected femoral pseudoanerysms remain controversial • Simple ligation & excision with debridement is the most common approach, with considerable risk of severe claudication, critical ischemia, and amputations in some individuals • Revascularization aim to avoid gangrene, maintain limb viability, and lower claudication rates, but need to accept the major risk of significant and life-threatening secondary complications
[1] Hussain MA, Roche-Nagle G. Infected pseudoaneurysm of the superficial femoral artery in a patient with Salmonella enteritidis bacteremia. Can J Infect Dis Med Microbiol. 2013;24(1):e24-e25 [2] Ting AC, Cheng SW. Femoral pseudoaneurysms in drug addicts. World J Surg. 1997;21(8):783-6 [3] Jayaramans et al. Mycotic pseudoaneurysms due to injection drug use: a ten-year experience. Ann Vasc Surg. 2012;26(6):819-24 [4] Saini et al. Infected pseudoaneurysms in IV drug abusers: ligation or reconstruction? Int J Appl Basic Med Res 2014;4:S23-26 [5] Brossier et al. New bacteriological patterns in primary infected aorto-iliac aneurysms: A single-centre experience. Eur. J. Vasc. Endovasc. Surg 2010;240;582-88 [6] Georgiadis GS et al. Surgical treatment of femoral artery infected false aneurysms in drug abusers. ANZ J. Surg. 2005; 75: 1005-1010 [7] Gan et al. Outcome after ligation of infected false femoral aneurysms in intravenous drug abusers. Eur. J. Vasc. Endovasc. Surg. 2000; 19:158-61 [8] Cheng SWK et al. Infected femoral pseudoaneurysm in intravenous drug abusers. Br. J. Surg. 1992; 79:510-12. [9] Tsao JW et al. Presentation, diagnosis and management of arterial mycotic pseudoaneurysms in injection drug users. Ann. Vasc. Surg. 2002; 16: 652-62 [10] Reddy DJ et al. Infected femoral artery false aneurysms in drug addicts: Evolution of selective vascular reconstruction. J. Vasc. Surg. 1986; 3: 718-24 [11] Benitez PR, Newell MA. Vascular trauma in drug abuse: patterns of injury. Ann Vasc Surg 1986; 1:175–181 [12] Arora S et al. Common femoral artery ligation and local debridement: a safe treatment for infected femoral artery pseudoaneurysms. J. Vasc. Surg. 2001; 33: 990-3 [13] Tan KK et al. Surgical management of infected pseudoaneurysms in intravenous drug abusers: single institution experience and a proposed algorithm. World J Surg. 2009 Sep;33(9):1830-5 [14] Yegane RA et al. Surgical Approach to Vascular Complications of Intravenous Drug Abuse. European Journal of Vascular and Endovascular Surgery 2006; 32(4):397-401 [15] Klonaris et al. Emergency stenting of a ruptured infected anastomotic femoral pseudoaneurysm. Cardiovasc Intervent Radiol 2007;30:1238-41 [16] Psathas et al. Management of a complicated ruptured infected pseudoaneurysm of the femoral artery in a drug addict. Case Reports in Vascular Medicine 2012; Article ID 434768 References
Q & A Ruptured Infected Femoral Artery Pseudoaneurysms in IV Drug Addicts
Investigation? • Active bleeding Urgent surgery • CT angiography • Duplex USG • Angiography • MR angiography
Limitations of current studies • High proportion of patients lost to follow-up • No study ever achieved complete post-surgery follow-up except in acutely symptomatic drug addicts • No fixed protocol for surgical management • Based on surgeon preferences • Mostly small scale, retrospective studies
YCH • 3 cases in past 6 months (Jan – June 2015) • 2 ligation + excision • 1 DAMA on POD1 • 1 discharged on POD3 • 1 death (hemorrhagic shock)
Prediction of need for revascularization? • No reliable subjective measures • Non-palpable pulses • Systolic pressure in PFA <40 mmHg (Padberg et al, 1992) • Lack of pedal Doppler scan signal after ligation or at test clamping of EIA (Arora et al 2001) • When patient is alert • Clinical assessment by pain in foot and calf, decreased power & range • Absence of pulse / positive Doppler signal does not necessitate immediate amputation
ABI • Normal 1.0 – 1.4 • <0.9 = PAD • >1.4 calcification / vessel hardening • 0.9-1 – acceptable • 0.8-0.9 – some arterial disease • 0.5-0.8 – moderate disease • <0.5 – severe disease