Download
1 / 21
210 likes | 639 Views
Orange Urine on Halloween. Eva Delgado, MD Morning Report. Overview. Case Presentation Indications for Referral/Admission Work-up based on Differential Discussion of Pathophysiology Treatment and Prognosis Take Home Points. Case Presentation.

E N D
Orange Urine on Halloween Eva Delgado, MD Morning Report
Overview • Case Presentation • Indications for Referral/Admission • Work-up based on Differential • Discussion of Pathophysiology • Treatment and Prognosis • Take Home Points
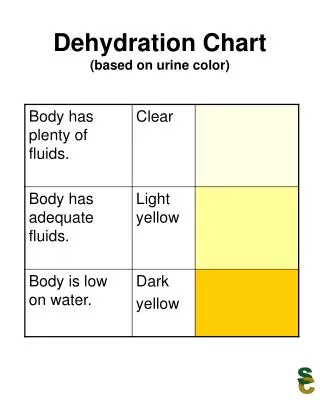
Case Presentation • 12 y/o F with OCD develops “orange” urine with sediment. • PMD advises watchful waiting.
Case Presentation • Orange urine persists x 4 days, so mom makes appointment with PMD. • PMD notes elevated BP, weight gain, and then orders one key test……….. • URINALYSIS: + hematuria, + proteinuria
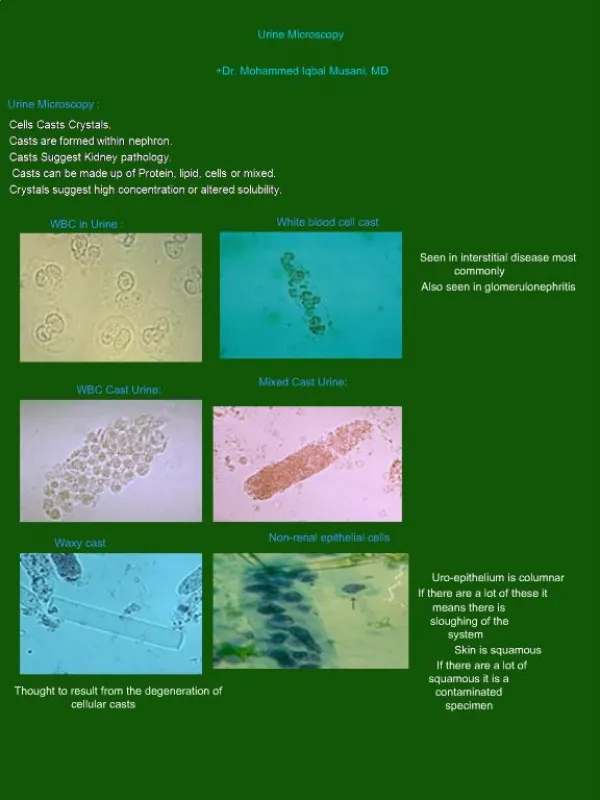
A Word on Urinalysis • UA with >/= 5 RBC/hpf on 3 samples over several weeks = HEMATURIA • Only UA can distinguish between confounders: • Myoglobin, hemoglobin, toxins, foods/coloring Massengill, Peds In Review, 2008
A Word on Disposition • Hematuria AND proteinuria • Proteinuria may be due to notable hematuria, BUT.. • Combination of both increases risk of renal disease • Hypertension • Can be a symptom of fluid overload warranting diuresis and further observation PMD sends patient to the ED….. Boineau and Lewy, Peds in Review, 1989. Simckes and Spitzer, Ped in Review, 1995.
Physical Exam in ED • Wt 60kg (↑ over last 6 mos) • VS: T 36.4, P 68, BP 146/80, R 20, 100% O2 • Gen: no distress • HEENT: no peri-orbital edema, MMM • Chest: CTA b/l • CV: RRR, no murmur • Abd: soft, NTND • Ext: slight erythema in skin folds, no edema
Differential and Work-Up • Urinalysis • Chemistry panel • CBC • C3, C4 • ASO +/- Throat swab • Imaging • Do you need a biopsy?
Thinking of Glomerulonephritis • Clues to look for in H&P: • Edema, discolored urine (in 30-50%), HTN due to ↓GFR and hypervolemia, oliguria • Clues to look for in UA: • + hematuria, + proteinuria, + casts (60-85%) • RBC dysmorphology implies glomerular damage • Sensitivity 95%, specificity 90% McCory, Peds in Review, 1983. Boineau and Lewy, Peds in Review 1989.
Glomerulopathy vs. Glomerulonephritis Silverstein, Laughing your way to passing the pediatric boards, 2008.
Laboratory Results • UA: 3+ blood, 2+ protein, 1+ LE, 0 nitrites, 11-20 WBC, numerous RBC, 1-3 granular casts • Chemistry: BUN/Cr = 17/0.8 • CBC: Hbg 11.3, HCT 32.5, MCV 79 • C3: 26 (86-184) • C4: 21.5 (20-59) • ASO: 2130 (<400 unit/ml); and + Rapid strep
Poststreptococcal GN • Most common type of Acute GN • Usually occurs in 5-15 y/o • 50% of cases are asymptomatic • Diagnosed by evidence of Group A Strep • ASO titers detectable 2-4 weeks s/p pharyngitis • Anti-DNase-B titers helpful in post-pyoderma type Simckes and Spitzer, Peds in Review 1995.
The Role of Grp A Strep • Nephritogenic strains of streptococci • Wall protein M12 in pharyngitis, M49 in pyoderma • These strains pose ~ 15% risk of PSGN approx 2 weeks after initial infection • Antibiotic treatment to prevent GN? Simckes and Spitzer, Peds in Review, 1995. Rodriguez-Iturbe and Musser, J Am Soc Nephrology, 2008
The Role of Grp A Strep • PANDAS = Post-infectious Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infection • Syndenham’s Chorea and Rheumatic Fever • OCD/Tic disorders shown to emerge or worsen with temporal relation to Grp A Strep infection • PANDAS patients may have higher susceptibility to Grp A Strep infection, + family h/o Rheumatic Fever Kurlan et al. 121 (6): 1188. (2008)Pediatrics
Considering the DDX of PSGN • Low C3 • 80-90% of PSGN cases have low C3 x 2 mos • Also seen in GN due to SLE • Consider MPGN if low C3 > 2 mos • MPGN can also present after infection • MPGN may also low C4 • Diagnose by biopsy TRAM-TRACKING McCrory, Peds In Review, 1983.
Considering DDX of PSGN • Normal C3: • IgA Nephropathy • Suspect if recurrent hematuria with URIs/Infections • Alport’s • + Family History • HUS or HSP can present with gross hematuria • Post-viral GN Boineau and Lewy Peds in Review 1989.
Treatment of AGN in General • Admit if HTN, edema, or signs of renal failure • Monitor/correct electrolyte anomalies • Treat HTN to avoid sequelae • Diuresis loop diuretics like lasix • Fluid and salt restriction • Anti-hypertensives like the Ca-channel blockers Simckes and Spitzer Peds in Review, 1995.
Treatment Specific to PSGN • Antibiotics to target Grp A Strep • Cultures often positive even if no symptoms, suggesting active infection • Treatment may milder course of PSGN • Epidemics of Grp A Strep may warrant ppx to prevent PSGN, especially in underdeveloped societies • Unclear/controversial role for impact on OCD Rodriguez-Iturbe and Musser, J Am Soc Nephrology, 2008
Prognosis and Sequelae • Good prognosis in children • CLOSE follow-up! • HTN resolves in ~ 1-2 weeks • C3 levels return to normal in ~ 6 weeks • Gross hematuria resolves in ~ 6 weeks • Microscopic hematuria resolves in ~ 1 year • Proteinuria resolves in ~ 6 months • Progression to renal dysfunction RARE McCrory, Peds in Review 1983.
Take Home Points • Urinalysis is KEY test to w/u discolored urine • UA with casts/dysmorphic RBCs = GN • HTN, edema, or renal dysfunction admit • Poststrep GN = most common, due to characteristics of Strep and/or patient • Treat Strep infection and co-morbidities • Guarantee follow-up
Works Cited • Boineau and Lewy, “Evaluation of Hematuria in Children and Adolescents,” Pediatrics in Review, 1989. • Kurlan et al., “Streptococcal Infections and Exacerbations of Childhood Tics and OCD Symptoms: A Prospective Blinded Cohort Study,” Pediatrics 2008. • Massengill, “Hematuria,” Pediatrics in Review, 2008. • Rodriguez-Iturbe and Musser, “The Current State of Poststreptococcal Glomerulonephritis,” Journal of American Society of Nephrology, 2008. • Simckes and Spitzer, “Poststreptococcal Acute Glomerulonephritis,” Pediatrics in Review, 1995. • McCrory, “Glomerulonephritis,” Pediatrics in Review, 1983.