Download
1 / 40
400 likes | 521 Views
Food and Nutrition Activities in the President’s Emergency Plan for AIDS Relief (PEPFAR). CAPT Pamela Ching, RD/LD, MS, SD Nutrition Medical Officer Division of Global HIV/AIDS Center for Global Health Centers for Disease Control and Prevention. Goals.

E N D
Food and Nutrition Activities in the President’s Emergency Plan for AIDS Relief (PEPFAR) CAPT Pamela Ching, RD/LD, MS, SD Nutrition Medical Officer Division of Global HIV/AIDS Center for Global Health Centers for Disease Control and Prevention
Goals • Background on food insecurity and undernutrition • Overview • Global Health Initiative (GHI) • President’s Emergency Plan for AIDS Relief (PEPFAR) • Food and Nutrition (F&N) activities • Assessments of food insecurity and malnutrition • Provision of therapeutic and supplemental foods to eliminate macro- and micro-nutrient deficiencies • Training clinical and community-based personnel
Food Insecurity “The limited or uncertain availability of nutritionally adequate, safe foods or the inability to acquire personally acceptable foods in socially acceptable ways.” (American Institute of Nutrition) “The right to adequate food is realized when every man, woman and child, alone or in community with others, has physical and economic access at all times to adequate food or means for its procurement.” (United Nations Committee on Economic, Social, and Cultural Rights, 1999)
Global Food Insecurity ~ 850 million people were food insecure last year (World Food Programme)
Undernutrition INTERVENTIONS CAUSES - Breastfeeding - Complementary feeding - Vitamin A - Zinc - Hygiene Immediate Health Food/nutrient intake Water/ Sanitation health services Access to food Maternal and child-care practices Underlying causes at household/ family level • - Agriculture • - Poverty Reduction • Income generation • Education • - Women’s empowerment • - Health Systems Strengthening INSTITUTIONS Basic causes at societal level POLITICAL & IDEOLOGICAL FRAMEWORK ECONOMIC STRUCTURE RESOURCES ENVIRONMENT, TECHNOLOGY, PEOPLE (Adapted from: United Nations Standing Committee on Nutrition News, 2008)
Undernutrition US Efforts Breastfeeding Complementary feeding Vitamin A Zinc Hygiene Health PEPFAR Food/nutrient intake GHI Water/ Sanitation health services Access to food Maternal and child-care practices Agriculture Poverty Reduction Education Health Systems Strengthening Income generation Women’s empowerment INSTITUTIONS Department of State POLITICAL & IDEOLOGICAL FRAMEWORK ECONOMIC STRUCTURE RESOURCES ENVIRONMENT, TECHNOLOGY, PEOPLE
“We cannot simply confront individual preventable illnesses in isolation. The world…demands an integrated approach to global health. We will not be successful in our efforts …unless we do more to improve health systems around the world…and ensure that best practices drive the funding for these programs.” President Barack Obama May 5, 2009
Global Health Initiative (GHI) • Six-year, $63 billion commitment by the US government to assist developing countries in reducing morbidity and mortality from HIV/AIDS, tuberculosis, malaria, and neglected tropical diseases • Objectives: • Achieve significant health improvements • Create an effective, efficient and sustainable platform for the delivery of essential health care and public health programs
GHI Goals • Nutrition: Reduce child undernutrition by 30% across assisted food insecure countries in conjunction with the President’s “Feed the Future” initiative. • HIV/AIDS: PEPFAR will support: • Treatment of > 3 million people with anti-retrovirals (ARVs) • Prevention of > 12 million new HIV infections • Care of > 12 million people, including 5 million orphans and vulnerable children
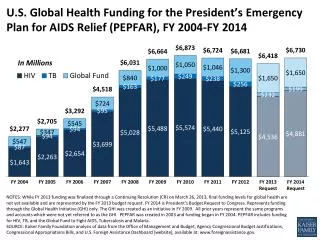
President’s Emergency Plan for AIDS Relief (PEPFAR) • 2003: Congress authorizes 5-year, $15 billion Program • A crucial component of US foreign policy • Program focused on provision of comprehensive HIV/AIDS prevention, care, and treatment using a multi-sectoral approach in developing countries most affected by the epidemic • 15 focus countries (12 in Sub-Sahara Africa; Haiti; Guyana; Vietnam) accounting for >50% global HIV/AIDS burden • 2009: 5-year reauthorization within GHI: $48 billion for HIV/AIDS, tuberculosis, and malaria
HIV/AIDS, Food, and Nutrition • “Slim Disease” - People living with HIV/AIDS (PLWHA ) typically present with advanced AIDS after chronic illness and >10% weight loss • Strong correlation between wasting and mortality before and during treatment • Food is often the most urgent need for PLWHA and their families • Anti-retroviral therapy (ART) and treatment for opportunistic infections improves appetite and nutritional status of most malnourished patients
Guiding Principles for PEPFAR F&N Programs • Support PEPFAR “3/12/12” goals • Strive to integrate nutrition assessment, counseling, and support (NACS) services within clinical care and treatment • Provide food and specialized nutritional supplements to target groups using defined eligibility criteria (“Food as Medicine”) • Be linked with food assistance and security programs supported by other initiatives or “wrap-arounds” (e.g., UN World Food Programme; USAID’s Title II, Food for Peace Program)
Target Groups for PEPFAR F&N Support • Orphans and vulnerable children (OVC), especially those under 5 years of age • HIV+ pregnant and lactating women in prevention of mother to child transmission (PMTCT) programs • People living with HIV/AIDS (PLWHA) in care and treatment programs
Food by Prescription (FBP) • Nutrition assessment, counseling, and support = NACS • FBP - program supporting NACS • Nutrition assessment: entry and “graduation” anthropometric and clinical criteria for malnourished and nutritionally vulnerable PLWHA, pregnant and lactating women and their infants enrolled in PMTCT programs, and OVC • Provision of nutrition education and counseling
Food by Prescription (FBP) • Therapeutic and supplementary feeding support • RUTF (Ready-to-use Therapeutic Food), e.g., Plumpy’nut • FBF (Fortified Blended Foods – grain and legume based flour/cereals • Sometimes: multi-micronutrient supplements • Instruction and supplies to support safe water treatment • Referral and support for household food security and livelihood assistance
Food Company • Food production • Delivery to hospital/clinic Hospital / Clinic VCT • Physician/Nurse • Symptom diagnosis • Integrated symptom treatment/management • Nutritionist/Health Worker • Assessment • Counseling • MN supplement & food prescription • Referral to clinical care & household food security Referral • Pharmacy • Food dispensing • Inventory control • Record keeping Inpatient • Lay Counselor • Nutrition education/ counseling • Peer support HBC/Community • Community Programs • Food security • Livelihood assistance • MCH Food by Prescription (FBP)
PEPFAR-Supported F&N Efforts • Basic FBP program implementation: • In operation: Malawi, Zambia, Haiti • Starting: Namibia, Ghana • Planning: Cote d’Ivoire, Mozambique, Vietnam • FBP with quality assessment and improvement evaluation activities: • Kenya, Tanzania, Ethiopia, Uganda
PEPFAR-Supported F&N Efforts • LIFT (LIvelihoods & Food Security Technical Assistance) Project • Provide household economic strengthening and livelihood assistance to food-insecure HIV/AIDS-affected families, including OVC • Technical assistance in Nigeria, Malawi, Kenya, Ethiopia, Rwanda, Mozambique, South Africa and Namibia.
Future PEPFAR-Supported F&N Efforts • PMTCT programs: greater emphasis on infant feeding practices which promote infant HIV-free survival in addition to prevention of peri-natal HIV transmission • Promote prolonged breastfeeding in conjunction with use of ART • Counseling on appropriate and timely weaning from breastfeeding and introduction of complementary foods • Establish local capacity to produce therapeutic and supplementary foods (e.g., RUTF; FBF; urban and rural gardens) • Establish globally-accepted food security and nutritional status indicators which are harmonized with HIV/AIDS status indicators
Acknowledgements • Nicholas Vogenthaler - Emory University • RoshellePayes and Eunyong Chung - USAID, Washington • Tonya Himelfarb – Office of the Global AIDS Coordinator, US Department of State • Tim Quick and Amie Heap – USAID, Washington
Food Security Food security = all people at all times have both physical and economic access to sufficient food to meet their dietary needs for a productive and healthy life. AVAILABILITY: sufficient quantities of food from household production, other domestic output, commercial imports or food assistance ACCESS: adequate resources to obtain appropriate foods for a nutritious diet, which depends on income available to the household, on the distribution of income within the household and on the price of food UTILIZATION/CONSUMPTION: proper biological use of food, requiring a diet providing sufficient energy and essential nutrients, potable water and adequate sanitation, as well as knowledge within the household of food storage and processing techniques, principles of nutrition and proper child care and illness management
More than 1/3 of children in Africa & Asia are underweight. Stunting remains a greater problem than underweight or wasting. Global Undernutrition
Issues to Address Concerning Undernutrition • Stunting and iron deficiency anemia have not been adequately addressed • Poor growth in many countries related to inadequate breastfeeding, complementary feeding, and infectious disease • Refocus on dietary quality, high levels of morbidity, and possibly intergenerational factors affecting linear growth. • Targeting of pregnant women and children under 2 – ‘window of opportunity’ – especially in communities with highest prevalence of stunting • Gross inequities throughout region and within countries: Rural vs. urban; indigenous vs. non-indigenous • Human resources and capacity constraints for health and nutrition
PEPFAR Five-Year Strategy(FY 2009-2013) • Transition from an emergency response to promotion of sustainable country programs. • Strengthen partner government capacity to lead the response to this epidemic and other health demands. • Expand prevention, care, and treatment in both concentrated and generalized epidemics. • Integrate and coordinate HIV/AIDS programs with broader global health and development programs to maximize impact on health systems. • Invest in innovation and operations research to evaluate impact, improve service delivery and maximize outcomes. (Executive summary of PEPFAR’s strategy: http://www.pepfar.gov/strategy/document/133244.htm)
Nutrition Implications of HIV/AIDS • Daily caloric needs: • Asymptomatic: 10% increase • Symptomatic: 20-30% increase • Children with weight loss: 50-100% increase • Daily protein needs: • Maintain at 12-15% of daily caloric intake (typically at least twice that of cereal- and tuber-based diets common in developing countries) • Micronutrients (essential vitamins/minerals) • At least daily recommended level s for non-HIV-infected individuals (which many such individuals as well s HIV/AIDS patients do not yet achieve) • Require high-energy, nutrient-dense foods
Recommended Elements for PEPFAR F&N Programs • Nutrition Care – Goal: Improved/Adequate Nutrition Status • Nutrition Assessment, Counseling & Support (NACS) • Assessment: • Anthropometric; Clinical; Dietary; Environmental (i.e., household food security) • Counseling: • Clinical (adherence to ART ) • Dietary (use of special therapeutic and supplemental foods; adherence to WASH and food safety practices) • Psychosocial • Support: • Food by Prescription; commodity support • Safe Water Treatment • Multi-micronutrient supplements • Referral to social services for livelihood and food security
Recommended Elements for PEPFAR F&N Programs • PMTCT – Goal: HIV-Free Survival • ART: HAART; Maternal/Infant Prophylaxis • Infant Feeding Counseling & Support • Postnatal Care: • Growth monitoring; • Basic child survival package (immunizations; routine micronutrient supplementation; insecticide-treated bednets; • Opportunistic infections: Cotrimoxizole; clinic referral) • Feeding Support • Maternal • Infant • Complementary • Replacement • Community Management of Acute Malnutrition (CMAM)
Recommended Elements for PEPFAR F&N Programs • Livelihoods and Food Security – Goal: Household Food Security • Food Production • (Re-) Employment • Involvement in income-generating activities • Vocational Training • Food Commodity Affordability
Nutrition Assessment, Counseling, and Support (NACS) • Clinical care and treatment services and F&N support are linked for PLWHA and OVC • Reciprocal impact between health & nutrition • Therapeutic and corrective model Preventive and chronic nutrition management model • PLWHA and women in PMTCT are linked to groups for treatment and F&N support, education, and counseling • Referrals for livelihood (income-generating) and food security support • Health system strengthening -- strengthens capacity of clinics and communities to provide NACS for all individuals, not just HIV/AIDS infected and affected
Nutrition Care PMTCT/ Infant Feeding Food Security Nutrition and HIV Indicators
Lessons Learned • Clinics where NACS is initiated are understaffed and overstretched. Quality Improvement (QI) efforts will be critical to finding efficiencies that allow integration of NACS within clinical services • Training of healthcare workers are necessary, but not sufficient –all training should be linked to QI efforts and the realities of Human Resources (HR) • Training should be decentralized, and individualized to the needs of each of the different types of healthcare workers
Lessons Learned • Prioritize provision of F&N program and services to the most vulnerable: • #1 - Infants and young children • #2 - Pregnant and lactating women in PMTCT programs • #3 - Adult PLWHA • Roll-out of NACS should precede initiation of FBP programs -- build ability to carry out NACS and secure commodities • Counseling of “Food as Medicine” in FBP leads to limited sharing of food by patient within his/her household, resulting in good weight recovery • Assessment and counseling , even without provision of therapeutic foods and supplemental food commodities improves nutritional status of patients • Linkage of F&N support to other community programs and public health surveillance results in improved nutritional and health outcomes at lower costs
Challenges in F&N Programming Integration and expansion of comprehensive NACS into other public health initiatives Linking clinical services with referral and support for food and livelihood assistance so as to produce sustainable food security among HIV/AIDS patients Balancing programming emphasis and resources for nutritional assessment and counseling with those needed for provision of food and feeding support
Challenges in F&N Programming • Balancing efforts to support food production among patients with support for (re-)employment, income generating activities, and other livelihood assistance • Balancing support and resources equitably among three vulnerable population groups: adult patients in care and treatment programs, women and infants supported in PMTCT programs, OVC