Download
1 / 21
210 likes | 225 Views
Bleeding in Patients Undergoing Percutaneous Coronary Interventions: A Risk Model From 302,152 Patients in the NCDR. Sameer K. Mehta MD, Andrew D. Frutkin MD, Sunil V. Rao MD, Fang–Shu Ou MS, Eric D. Peterson MD, MPH, John A. Spertus MD, MPH, Steven P. Marso MD, on behalf of the NCDR

E N D
Bleeding in Patients Undergoing Percutaneous Coronary Interventions: A Risk Model From 302,152 Patients in the NCDR. Sameer K. Mehta MD, Andrew D. Frutkin MD, Sunil V. Rao MD, Fang–Shu Ou MS, Eric D. Peterson MD, MPH, John A. Spertus MD, MPH, Steven P. Marso MD, on behalf of the NCDR The Mid America Heart Institute and Duke Clinical Research Institute. American Heart Association Scientific Sessions – November 5, 2007
Presenter Disclosure Information Sameer K. Mehta MD et al. Bleeding in Patients Undergoing Percutaneous Coronary Interventions: A Predictive Model From 302,152 Patients in the NCDR. No authors report any disclosures or conflicts of interest.
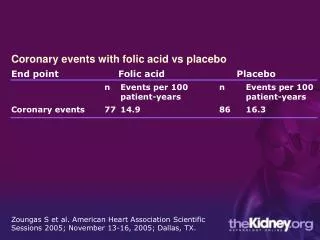
Bleeding and PCI The incidence of major bleeding in patients undergoing PCI is as high as 5%. Bleeding events have been associated with an increased incidence of adverse outcomes, including death, MI, and stroke. A tool that helps physicians assess the risk of bleeding in PCI patients may allow physicians to individualize antithrombotic and antiplatelet therapy while mitigating the risk of bleeding. Goodman et al. Circulation 2003. Eikelboom et al. Circulation 2007. Rao et al. American Journal of Cardiology 2005.
Aims To determine the risk factors of bleeding in a large, contemporary, real-world cohort of patients undergoing PCI. To develop a risk model for bleeding. To test the validity of this risk model in clinically important subgroups.
Methods Version 3.04 of NCDR Cath-PCI Registry Contains data from PCI procedures performed from Jan. 1, 2004 to March 31, 2006 at over 600 U.S. hospitals. Exclusions: - Non-index PCI - Patients who died same day as PCI - Patients with missing bleeding data - Centers that did not report any bleeding events
Methods (2) Final study population: 302,152 patients 302,152 PCI procedures 440 U.S. hospitals Determined predictors of bleeding with generalized estimating equation models. Models adjusted for age, sex, weight, GFR, PCI status, presence of ACS, cardiogenic shock, intra-aortic balloon pump treatment, history of MI, diabetes, cerebrovascular disease, peripheral vascular disease, hypertension, COPD, prior PCI, NYHA class, prior valve surgery, Caucasian, prior CHF, smoker, family history of CAD, EF, dyslipidemia, prior CABG, and CHF.
Methods (3) Risk model training set. 241,512 patients (80% of total) Risk model validation set 60,640 patients (20% of total) Variable selection via backward selection and clinical judgment Goodness of fit determined by calibration plot Discrimination assessed by c-statistic Risk model tested in various clinically meaningful subgroups
NCDR Bleeding Definitions Primary Endpoint: Bleeding from any source Percutaneous entry site: during hospitalization; transfusion and/or cause a drop in hemoglobin >3.0 g/dl; hematoma >10cm for femoral access, >2cm for radial access, or >5cm for brachial access. Retroperitoneal: transfusion and/or cause a drop in hemoglobin >3.0 g/dl.
NCDR Bleeding Definitions (2) GI: transfusion and/or cause a drop in hemoglobin >3.0 g/dl. GU: transfusion and/or cause a drop in hemoglobin >3.0 g/dl. Other/Unknown: During hospitalization transfusion and/or cause a drop in hemoglobin >3.0 g/dl.
Results Incidence of Bleeding in Training Set 2.5%
Risk Factors for Bleeding- Adjusted Analysis All p values <0.001
Overall Model Predicted Bleeding (%) N= 60,640 C Statistic =0.73 Observed Bleeding (%)
Subgroup Analyses Predicted Bleeding (%) N= 30,872 C Statistic =0.72 N= 9,130 C Statistic =0.70 Observed Bleeding (%)
Elective PCI Patients Predicted Bleeding (%) N= 29,733 C Statistic =0.67 Observed Bleeding (%)
Antithrombotic Therapy Unfractionated Heparin plus IIb/IIIa Unfractionated Heparin Predicted Bleeding (%) N= 22,666 C Statistic =0.72 N=24,969 C Statistic =0.73 Observed Bleeding (%)
Antithrombotic Therapy Low Molecular Weight Heparin Direct Thrombin Inhibitors Predicted Bleeding (%) N= 10,108 C Statistic =0.68 N= 19,316 C Statistic =0.73 Observed Bleeding (%)
Conclusions Identified risk factors for bleeding in PCI patients Developed a risk model that predicted the risk of bleeding in patients undergoing PCI Model performed well in various clinically important subgroups
Limitations Bleeding definitions differ between NCDR and TIMI/ GUSTO Low reported incidence of bleeding events
Future Directions Risk Score for Bleeding. Implementation of predictive model/ risk score into randomized studies of patients undergoing PCI.