Download
1 / 60
660 likes | 1.24k Views
子宫肌瘤 Myoma of uterus. 王世宣 ( Shixuan Wang ) Department of OB/GYN Tongji Hospital Tongji Medical College of HUST. Topics today. 发病相关高危因素 High risk factors 分类 Classification 病理 Pathology 肌瘤变性 Degeneration of uterine myoma 临床表现 Clinical manifestation

E N D
子宫肌瘤Myoma of uterus 王世宣 (Shixuan Wang) Department of OB/GYN Tongji Hospital Tongji Medical College of HUST
Topics today • 发病相关高危因素High risk factors • 分类Classification • 病理Pathology • 肌瘤变性Degeneration of uterine myoma • 临床表现Clinical manifestation • 诊断及鉴别诊断Diagnosis and differential diagnosis • 治疗Management
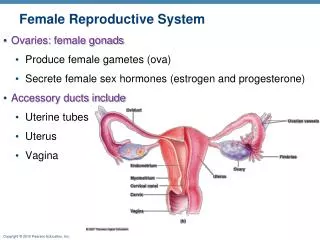
Most common benign tumor in female genitalia! Myoma of uterus Female Internal genitalia
MYOMA OF THE UTRUS-- in various region of uterus
General consideration • Terms: Myoma, leiomyoma, fibroid, fibroid tumor • Consists of: smooth muscle tissue + connective tissue • The most common benign tumor in female genital organs 20% of women over 30; 25% of women over 40 • Commonly seen in women of age: 30-50; 40- 50 yrs old with peak incidence Rare in girls under 20; shrink after menopause
High risk factors (1) • Cytogenetic factors • Female Hormones • Growth Factors • Molecular factors The exact causes remain unclear
High risk factors (2) • Cytogenetic factors: 20%- 50%, cytogenetic abnormalities (chromosome) family history • Female Hormones: Estrogens ↑, ER ↑ Hypersensitivity to estrogen Progestin ?
High risk factors (3) • Growth Factors: Epidermal growth factor (EGF) Insulin-like growth factor (IGF)-I Basic fibroblast growth factor (BFGF) • Cellular and Molecular factors: Hypothesis:stem cells monoclonal → single myoma polyclonal → multiple myomas
Stem cell(s) of myoma Pathogenesis of uterine myoma Estrogen High ER hypersensitivity Myoma of uterus Smooth muscle cells Cytogenetic background Growth factors
Classification of myoma of uterus Originate in the myometrium of uterus • 按肌瘤生长部位Classified by anatomic location • 按肌瘤与肌层关系Classified by relationship with myometrium
Classification- by the location: • 宫体肌瘤Corporeal myoma: 90% • 宫颈肌瘤Cervical myoma: 10%
Classification- by the relationship with myometrium • 肌壁间Intramural myoma: 60 % -70 % • 浆膜下Subserous myoma : 20% • 粘膜下Submucous myoma : 10 % -15%
Submucous ( / intracavitary) Subserous Submucous + Intramural + Subserous Submucous + intramural Subserous
Pathology • Gross view (Naked eye appearance) • Microscopic features
Pathology – gross view • Mass: Spherical, solid, hard; grey-white; pseudocapsule; often multiple • Section: paler, harder and more fibrous than the normal uterine myometrium (wall)
Pathology - Microscopic features • Smooth muscle cells arising from mostly myometrium, or endometrium of blood vessels • Composed of unstriped, interlaced bundles of smooth muscle and fibrous tissue • Condensed nuclei, mitotic activity
Fig. 1 100× left:normal; right:myoma with interlaced bundles of smooth muscle tissue fig. 2 100× Uterine myoma fig. 3 200× Uterine myoma
肌瘤变性Degeneration of myoma • Atrophic • hyaline degeneration • cystic degeneration • red degeneration • malignant transformation: mainly sarcomatous change • Others: myxomatous (fatty), septic, calcific (calcareous)
Hyaline degeneration • The commonest change seen in myoma. • caused by a gradual inadequacy of the blood supply.
Cystic degeneration • not uncommon, especially after the menopause • due to liquefaction of the areas of hyaline change.
Red degeneration • The affected area resembles raw meat and is stained red. • most freguently seen during the pregnancy and in postpartum.
Malignant change • 0.1%- 1% of cases • Most likely to be seen in large tumors. • More typical in older patients, especially postmenopausal patients • Presented with rapidly enlarging uterine mass and postmenopausal bleeding. • Metastasis occurs rapidly
症状Symptoms • Abnormal vaginal bleeding:the most common presenting symptom; hypermenorrhea(经量过多及经期延长) • Lower abdominal mass:usually asymptomatic • Vaginal discharge ↑ • Pressure effects: • Others:abdominal pain, infertility, secondary anemia
Symptoms – Abnormal vaginal bleeding (1) • Submucous myoma: almost 100%, quite small tumors can lead to severe anemia. • Intramural tumors: increasing of blood loss; prolonged period • Subserous growths: do not affect the menstrual loss.
Symptoms – Abnormal vaginal bleeding (2) Mechanisms for increased bleeding: • Alteration of normal myometrial contractile function • Inability of the overlying endometrium to respond to the normal E/P menstrual phases. • Pressure necrosis of the overlying endometrial bed.
Symptoms – abdominal mass • Sometimes the first thing that the patient notices. • Asymptomatic: not tender and rarely gives rise to pain.
Symptoms – Pelvic pressure • Against bladder (frequency and retention of urine) • Against rectum(constipation) • Against parauterine tissues: pain or discomfort
Symptoms – abnormal Vaginal discharge • 42% • ↑Area of uterine cavity • Pelvic congestion • Complications of submucous myoma
Symptoms – pelvic Pain not a common symptom, when it occurs: • Some complication of myoma such as, degeneration or torsion • Endometriosis • Pelvic inflammatory disease
Symptoms – others • Infertility:30%patients with myoma • Spontaneous abortion:4 :1 • Secondary Anemia:
体征Signs Vary with the size,site (region/ location), number, and complication of myomas. • abdominal examination • pelvic examination
Signs -Abdominal mass • ﹤3 months gestational age:not palpable • > 3 months gestational age: In the middle of the lower abdomen, irregular, hard, nodular
Signs -Pelvic mass • Intramural:enlargement of uterus; irregular, single or multiple nodules on the surface • Subserous:spherical, nodular masses • Submucous: symmetrical enlargement of the uterus ,extrusion of myoma into cervical canal even vagina
诊断Diagnosis • History: reproductive age • Symtoms: • Signs: • Ancillary tests: Ultrasonography Hysteroscopy Laparoscopy Dilation and curettage HSG
Essentials for diagnosis • Bleeding: hypermenorrhea, metrorrhagia, dysmenorrhea • Mass: irregular enlargement of the uterus (usually asymptomatic); solid, spherical, and nodular • Pain: from torsion or degeneration • Pressue symptoms: from neighboring organs (large tumors)
Diagnosis- ancillary test • Pelvic ultrasound the most commonly used for confirmation of uterine myomas
Submucous myoma Subserous myoma
Ancillary test -Hysteroscopy Ancillary test -Laparoscopy
Differential diagnosis (1) • Other conditions which give rise to a mass in the pelvis(盆腔包块) Adenomyoma Ovarian tumors Inflammatory mass in the pelvis Pregnancy Abnormality of uterus
Differential diagnosis (2) • Other conditions which cause metrorrhagia(子宫出血) Adenomyoma Endometrial polyp of uterus Carcinoma of the uterus: endometrial, cervical Dysfunctional uterine bleeding
治疗Management • Follow up • Drug therapy • Surgical management: hysterectomy;myomectomy • Others: Embolisation of myoma ; myolysis
Treatment - Follow up The majority of patients with uterine myomas do not require surgical treatment. • Age: Patients in the late reproductive or perimenopausal years. • Small and asymptomatic • Management: repeat pelvic examinations and assisted by serial pelvic ultrasound measurements • Every 3 - 6 months.
Management - Drug therapy Indications: • Perimenopausal women • small myoma (﹤2 months) • Asymptomatic, or with mild symptoms • Couldn’t tolerate surgery
Management - Drug therapy Mechanisms: • Pharmacologic inhibition of effects of estrogen • Inhibit the function of H-P-O axis • Commonly used for 3 to 6 months.