Download
1 / 55
550 likes | 707 Views
4. Palpation of masses the masses of abdomen may be caused by enlarged organ ectopic organ cyst carcinoma inflammatory tissues enlarged lymphnode.

E N D
4. Palpation of massesthe masses of abdomen may be caused by enlarged organ ectopic organ cyst carcinoma inflammatory tissues enlarged lymphnode
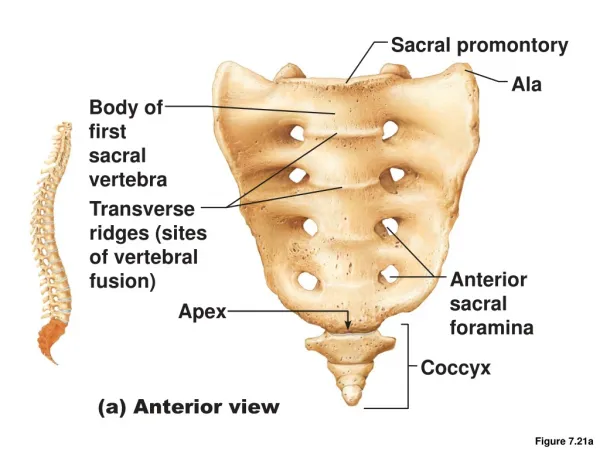
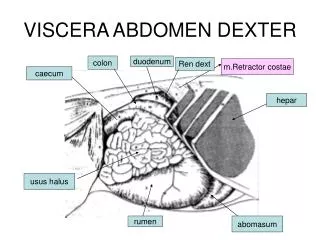
(1)Normal masses of abdomentendon of abdominal rectus lumber vertebral body sacral promontory sigmoid colon transverse colon cecum
(2).Abnormal mass of abdomenwhen you palpate the mass of abdomen you should describe the location size contour consistency tenderness pulsationmobility
The location of massThe mass usually originate from located organ, where you find a mass where the organ has lesion. If the location of mass is variable, the mass may originate from omentum, mesentery, or with stalk.
big mass without intestinal obstruction, the mass originate from mesentery peritoneum omentum postperitoneum
The size of massThe mass should be measured with a ruler to see how big it is, but sometimes the measurement is difficult, such as deep mass, small mass so you can estimate the size of mass, comparing with something like peanut, bean, egg, fist, baby`s head and so on.
Big mass usually indicate cyst such as ovarian cyst, hepatic cyst or polycystic kidney. Intestinal tumor usually accompanied with intestinal obstruction. Mass with variable size indicates spasm of intestinal segment.
The contour of mass※ the outline of mass is clear or not ※ the surface is smooth or not ※ the margin is sharp or blunt ※ round and smooth mass indicate a cyst
※ Irregular, nodular, hard mass indicate malignant tumor ※ A soft cystic mass in right hypochondrial region indicate distended gallbladder ※ A mass with notch in left upper quadrant indicate splenomegaly
The consistency of mass※ soft mass cyst, abscess ※ middle hard inflammatory mass ※ hard tumor the tenderness of mass※ severe tenderness inflammatory mass ※ light tenderness tumor
The pulsation of mass※ abdominal aneurysm or a mass next to the aorta ※ enlargement of liver with pulsation tricuspid valve incompetence
The mobility of mass※ a mass move with respiration it maybe from liver, spleen, stomach, kidney, gallbladder or transverse colon ※ a mass can be moved with hand it may be from stomach, intestine or mesentery
※ A mass can be moved easily and widely it may be from a tumor with a stalk wandering kidney wandering spleen ※ A mass can not be moved it may be from postperitoneal or inflammatory mass
5. Fluid wave thrillwith the patient in supine position, the examiner’s left hand is placed on the patient’ s right flank, an assistant (another person) places one hand on the middle of the abdomen to prevent the transmission of any wave through the tissues of the abdominal wall
The examiners’s right hand then lightly taps the left flank of the patient, in the presence of a significant amount of ascites, a wave will be transmitted through the fluid to the examiner’s left hand as a sharp impulse.
Succussion splashthis examining method can check for retention of gastric fluid. If succussion splash is positive after meal 6-8 hours indicating pyloric obstruction
Percussion can check for the presence of abdominaldistention, tumor, fluid, enlargement of viscera.percussion tone of abdomen liver spleen dullness flatness remains tympany
normal liver upper limit 5th intercostal space lower border --costal margin diameter of dullness 9-11cm enlargement of liver dullness hepatitis, hepatic carcinoma hepatic cyst hepatic abscess hepatic engorgement
Decreased liver dullness cirrhosis of liver, hepatonecrosis absence of liver dullness perforation of hollow viscus interposition of hepatic flexure of colon percussive pain of liver hepatitis hepatic abscess percussive pain of gallbladder cholecystitis
Percussion of spleennormal left midaxillary line 9th –11th intercostal space width 4-7cm enlargement of splenic dullness: splenomegaly
Percussion of kidneypercusive pain of kidney nephritis glomerulonephritis pyelothiasis perirenal abscesspercussion of bladder distended bladder dullness disappear after urination
Percussion of ascitesshifting dullness >1000ml elbow-knee position check for small amount ascites
differentiate massive ovariocyst from ascites ovariocyst dullness locate center abdomen no shifting dullness ruler pressing test (+)
bowel soundnormal 4-5times /min increased >10times acute intestinitis, loud high-pitched tinkling quality: intestinal obstructiondecreased or disappeared: acute peritonitis, intestinal paralysis, electrolyte disorder
vascular bruitsystolic bruitpartial occlusion of renal artery above umbilicus left or right side hepatic cancer lesion areaabdominal aneurysm or partial occlusion of abdominal aorta
Vein bruitperiumbilicus, upper abdomen or over the liver: continuous humming sound, seen in portal hypertension caused by cirrhosis of liver Friction rubover the spleen or over the liver perisplenitis caused by spleen infarction perihepatitis
Scratch sound exploration of hepatic lower edge auscultary percussion auscultary scratch exploration of small quantity of ascites about 120 ml
Gastric and Duodenal Ulcer In etiology, gastric and duodenal ulcer always have relation to hydrochloric acid and pepsin, so they are also called Peptic Ulcer
Symptoms Chronic pigastric pain is main symptom of peptic ulcer The pain has following features
1 Location and Extent The pain from gastric ulcer is just under xiphoid or left, but duodenal ulcer is located in the middle of epigastrium or right. The extent of the pain is just like a palm size.
2 The character of pain The character of pain is frequently described as burning, blunt or hunger pain. The pain is continuous, often lasting 1-4h.
3 Chronicity and Recurrence of peptic ulcer, some patients with peptic ulcer are reported annual recurrence of pain during particular seasons, such as spring or autumn, especially early spring or late autumn