Download
1 / 33
350 likes | 804 Views
RECTAL CARCINOMA. Rectum The rectum is about 12 cm long & upper part breath 4 cm Present in pelvic cavity. Position & Extent begins opposite Sacral Vertebra 3 as continuation of sigmoid colon passes downwards, following curve of sacrum & coccyx

E N D
Rectum • The rectum is about 12 cm long & upper part breath 4 cm • Present in pelvic cavity
Position & Extent • begins opposite Sacral Vertebra 3 as continuation of sigmoid colon • passes downwards, following curve of sacrum & coccyx • Then extends downwards forward about 2-3 cm in front & below tip of coccyx • It abruptly turns downwards & backwards & is continuous with anal canal at anorectal junction
External Apperance The rectum can be distinguished by • absence of mesentery & appendices epiploicae • absence of sacculations • teniae coli to form longitudinal muscle coat
Interior of Rectum Mucous membrane of empty rectum shows two types of folds Longitudinal fold: - Are transitory. • Present in lower part of empty rectum & obliterated by distension Transverse fold - Permanent • More marked in distended rectum Upper fold – • Near the upper end of rectum & projects from Rt. or Lt. Wall Middle Fold • Largest & most constant lies in upper end of rectal ampulla & projects from anterior & Rt. Walls Lowest Fold • Lies 2.5 cm below middle fold & projects from left wall
Blood Supply Artery • sup rectal art - Continuation of Inferior mesenteric artery • middle rectal art - Branch of Internal Iliac Artery • median sacral art - Branch of Abdominal Aorta
Venous Drainage • follow arteries • however free anastomosis exist between the superior, middle & inferior rectal veins Nerve Supply • Sympathetic from L1, L2 • Parasympathetic from S2-S4
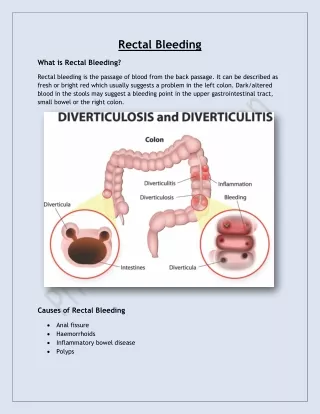
AETIOLOGY • Red meat and saturated fatty acids • Alcohol and smoking • Familial adenomatous polyp • IBD • HNPCC(heridatory Non Polyposis Colorectal Cancer) • Family history of rectal carcinoma
PATHOLOGY #HISTOLOGICALLY • Adenocarcinoma #GROSS • Ulcerative • Papilliferous • Infilterative • Annular
SPREAD • Local spread • Initially circumferentially and later spreads out to muscular coat and peri-rectal tissue. • Then to prostate,bladder,seminal vesicles in males and ureters and vagina in female. • Posteriorly into sacrum and sacral plexus. • LYMPHATIC SPREAD • Along the colonic lymph nodes • In mid-rectum----rectal and mid-rectal nodes
VENOUS SPREAD • Liver 35%, lungs 20%, adrenas 10% • PERINEURAL SPREAD
STAGING • MODIFIED DUKE’S STAGING • A.growth limited to rectal wall • B1.growth extending into extra rectal tissue but no lymph nodes spread • B2.invading muscularis mucosa • C.lymph nodes secondaries • D.distant spread to liver, lungs,bones,brain
TNM-STAGING • Tx—primary not assesssed • T0—no primary tumour • Tis-- carcinoma in situ • T1-- invasion to submucosa • T2-- invasion to muscularispropria • T3-- invasion of subserosa • T4 --involvement of visceral peritoneum • N0-- no nodal spread • N1--1----3 nodal spread • N2-- 4 or more nodal spread • Mo-- no distant spread • M1-- distant spread present
CLINICAL FEATURES • Bleeding per rectum------earliest symptom • Spurious diarrhea • Tenesmus • Sense of incomplete evacuation • May present as piles -------due to proximal venous congestion • Altered bowel habit • Anemia & malnutrition • Urinary symptoms due to bladder infiltration • Ascites and liver secondaries
INVESTIGATIONS • 1)ABDOMINAL EXAMINATION • Normal in early cases • Advanced annular tumour at rectosigmoid junction----------signs of int.obstruction. • Palpable liver----metastasis • Ascites ---secondary deposits to peritoneum
2)PER RECTAL EXAMINATION • DRE---nodule with an indurated base • Bimanual examination---may be possible to feel the lower extremity of a carcinoma situated in rectosigmoid junction • Carcinoma in lower 3rd of rectum------lymph nodes 1 or more hard,oval swellings in the mesorectumposteriorly or posterolaterally above the tumour • In females----vaginal examination is must
3)PROCTOSIGMOIDOSCOPY • Will always show carcinoma--------rectum should be empty before hand • 4)BIOPSY • Using biopsy forceps via a sigmoidoscope---will confirm the diagnosis • 5)COLONOSCOPY • To exclude other tumours. • 6)ultrasound
MANAGEMENT • A) PRE-OPERATIVE PREPARATION • Mechanical bowel preparation • Counselling and siting of stomas • Correction of anaemia and electrolye disturbances • Cross-matching of blood • Prophylactic antibiotics • DVT prophylaxis • Insertion of urethral catheter
B)SURGERY • 1)Abdomino-perineal resection(APR-OPERATION) • Sigmoid,descending colon and upper rectum is mobilised per-abdominally • Anal canal with perianal and perirectal tissue are dissected per anally • Retained colon is brought out as end colostomy in LIF. • 3 TYPES------- • MILES---abdomen 1st and perineum later • Gabriel----perineum 1st and abdomen later • Lioyd-davis----combined
2)ANTERIOR RESECTION. • Done in growths located in the mid and upper part of rectum. • CRITERIA • 1-UPPER AND MIDDLE THIRD RECTAL GROWTH • 2-ABOVE PERITONEAL REFLECTION • 3-WELL-DIFFERENTIATED TUMOUR • 4-LESS THAN 4CM SIZE TOMOUR • 5-TI-N0OR T2-NO TUMOUR
3)HARTMANN’S OPERATION • PALLIATIVE PROCEDURE DONE IN ELDERLY • Rectal growth is resected and upper end of rectum is closed completely • Proximal colon is brought out as end colostomy. • 4)PELVIC EVISCERATION • 5)PALLIATIVE COLOSTOMY
C)RADIOTHERAPY -useful when growth is below the level of peritoneal reflection D)CHEMOTHERAPY -5-FU, folinic acid etc E)LASER PHOTOCOAGULATION