Download
1 / 44
590 likes | 1.36k Views
Acute Lymphoblastic Leukemia An Overview. Aziza Shad, MD. Case 1. History: 3yo boy presents to Emergency Department with a 5 day history of back pain and pain/difficulty walking On exam: Febrile with pallor, bruising, petechiae, mild hepatosplenomegaly Labs:

E N D
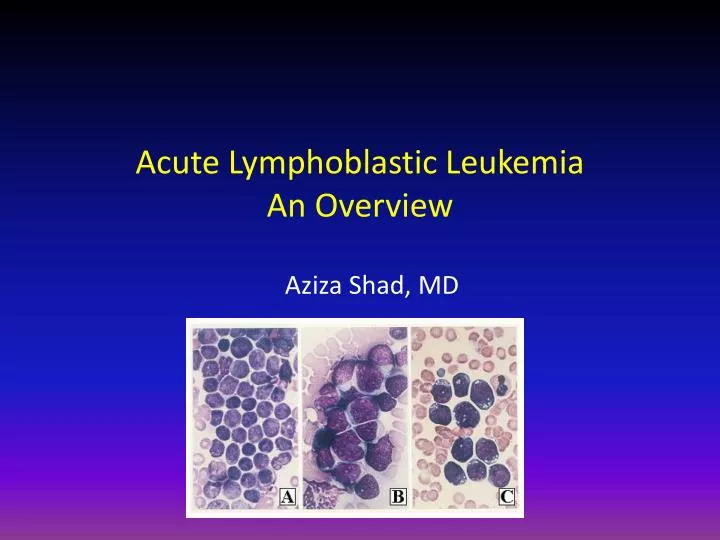
Acute Lymphoblastic LeukemiaAn Overview Aziza Shad, MD
Case 1 • History: 3yo boy presents to Emergency Department with a 5 day history of back pain and pain/difficulty walking • On exam: Febrile with pallor, bruising, petechiae, mild hepatosplenomegaly • Labs: CBC: Hgb 6.0g, Hct 18.0, Plts 11k, WBC 13.6 (10p, 60l, 24 atypical lymphocytes, 6 blasts) ANC 136 CHEM: K normal, Uric acid 7.0 ↑, LDH 2200 ↑ • CXR: Reported as normal
Peripheral smear Blasts with scant cytoplasm and prominent nucleoli Maslak, P. ASH Image Bank 2004;2004:101159
Bone marrow aspirate and biopsy • BMA: Blasts have a high nuclear to cytoplasmic ratio and lack granules in the cytoplasm • BMBx: Bone marrow architecture is replaced by monotonous population of blasts Maslak, P. ASH Image Bank 2002;2002:100400 and 100526
Maslak, P. ASH Image Bank 2004;2004:101200 Diagnosis? Acute Leukemia (most likely ALL)
Making the diagnosis: Morphology and Immunophenotype
Morphologic classification – French American British (FAB) subtypes L1 – 85% Small, uniform cell size Fine, homogeneous chromatin Scant cytoplasm Inconspicuous nucleoli L2 – 14% Large, heterogeneous cell size Irregular, clefted nuclei Variable amount of cytoplasm Nucleoli usually visible L3 – 1% Large, homogeneous cell size Prominent vacuolization Basophilic cytoplasm Nucleoli usually visible
Introduction • Leukemia accounts for about a third of all childhood cancers • About 80% of children with leukemia have ALL • 17% have AML • The remainder have rare forms of chronic leukemia
Pediatric Acute Lymphoblastic Leukemia • Most common cancer of childhood • Affects children from 0 -20 years • Peak incidence is between 3 -6 years • Untreated, life expectancy is days to weeks • Modern risk-based therapy has brought the cure rate up to 75 -85% • for some sub-groups, the cure rate is close to 90%, for others, it is < 20%
Epidemiology of Pediatric ALL • Most common form of childhood leukemia • 2,500-3,000 children annually in U.S. (3 per 100,000) • Sibling relative risk is 2-4x • Monozygotic twin concordance 25% - highest in infancy, no increased risk after 7 years of age • mechanism in monozygotic twins is shared in utero circulation, with transfer of preleukemic from one twin to the other
Pathophysiology • Most cases – cause unknown • Inherited genetic syndromes: • Downs syndrome, Bloom’s syndrome, Nijmegen breakage syndrome, ataxia telangiectasia • Environmental exposures • Ionizing radiation, benzene, prior chemotherapy • Other possible environmental influences • High birth weight, parental tobacco/alcohol, maternal diet, exposure to pesticides or solvents, prenatal vitamins (protective)
Clinical Presentation • Symptoms directly related to marrow infiltration • Decreased WBC : fevers, infections • Decreased RBC :signs and symptoms of anemia • Decreased platelets: bruising, bleeding • Marrow infiltration: bone pain, limp • Extramedullary infiltration : lymphadenopathy, hepatosplenomegaly, mediastinal mass
Remember… • A given case may have several symptoms or only a few • A normal CBC does not rule out leukemia! • Back pain/limp in pediatrics is a red flag and requires work-up • Before treating any child with steroids for any reason, stop and think about whether leukemia is in the differential diagnosis
Differential Diagnosis • Non Malignant conditions: • Juvenile rheumatoid arthritis • Infectious Mononucleosis • ITP • Pertussis and Parapertusis • Aplastic Anemia • Other viral illnesses
Differential Diagnosis • Malignancies: • Neuroblastoma • Retinoblastoma • Rhabomyosarcoma • NHL • Other small round blue cell tumors • Hyper-eosinophilia, other aplastic presentations
Standard Work-up for ALL • History and Physical Exam • CBC, electrolytes, LDH, Uric acid • Peripheral smear • Chest X-Ray • Bone marrow aspirate and biopsy with special stains • Immunophenotyping ( flow cytometry) • Cytogenetics • Molecular diagnostics
Immunophenotype Side-scatter CD10 CD19 CD45 CD138 CD22
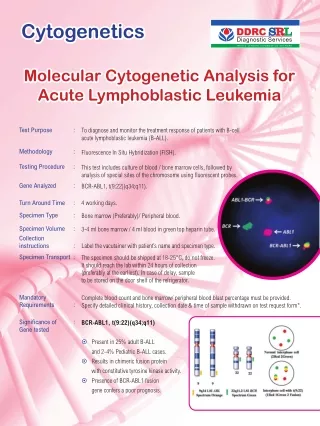
Molecular genetics • Favorable risk • TEL-AML1 (ETV6-RUNX1) fusion, t(12;21) • Hyperdiploidy (esp triple trisomies – chr 4, 10, 17; or double trisomies – chr 4, 10) • High risk • Philadelphia chromosome, t(9;22) • MLL rearrangement (11q23) • Hypodiploidy (<44 chromosomes) fusion signal
Back to our patient… • Received hydration, PRBC and platelet transfusions, tumor lysis lab monitoring and prophylaxis (allopurinol) • Consented to start induction chemotherapy • Bone pain and fevers resolve within a few days, discharged home to follow up for ongoing outpatient chemotherapy • What is his prognosis?
Cure Rates • Over the last 50 years, survival rates for childhood cancer have risen from 10% to almost 80% • Remarkable progress has been made in the past decade in the treatment and understanding of leukemia • Collaborative clinical trials implementing risk-stratified therapy have dramatically improved cure rates in ALL • Outcome in ALL has gone from a 6-month median survival to an 80% overall cure rate
100 80 60 40 20 Years of Diagnosis Number of Children 1995-97 1,299 1993-95 1,585 1989-93 3,402 % Survival 1983-89 3,711 1978-83 2,984 1975-78 1,313 1972-75 936 1970-72 499 1968-70 402 0 2 6 8 10 4 Total Number of Patients Treated: 16,131 Years after Study Entry Legend: Survival of CCG Patients with Newly-Diagnosed Acute Lymphoblastic Leukemia, 1968-1997. Bleyer A, Hather N, Personal Communication
Prognostic Factors in Childhood ALL • Age • WBC count at presentation • Immunophenotype • Recurrent chromosomal abnormalities • Response to initial therapy • These prognostic factors have been used to stratify therapy following induction remission • Gene expression analysis • Pharmacogenomics
Risk adapted therapy for Pediatric ALL • Standard, high or very-high risk groups • Patients with ‘high risk’ features get intensified chemotherapy • Patients with ‘very-high risk’ features are candidates for BMT • ‘Low risk’ group being studied – reduced intensity treatment
Prognostic Factors in Childhood ALL • Clinical and Lab features • Leukemia cells characteristics • Response to initial therapy
Prognostic Variables • Clinical and Lab Variables: • Age: • 1-9 yrs Best outcome 5 yr EFS 88% • 10-15 yrs 73% • >15 yrs 69% • < 12 mths 44% • < 6 mths poor outcome • Infants: Poor outcome • MLL gene, Increased WBC, CNS Leukemia • CD10 Negative • Poor initial response Pui et al, Lancet 2008
Prognostic Variables • Clinical and Lab Variables: • WBC Count at Presentation: • Increasing WBC confer a poor outcome especially in patients with Precursor B-cell ALL • T-cell ALL patients with WBC > 100k have a higher risk of CNS relapse
Prognostic Variables • Leukemic Cell Characteristics: • Immunophenotype: • Precursor B ALL: CD19, CD10 (cALLa), HLA-DR 80%- 85% of ALL 80% CD10 positive • Early pre-B (no sIg or cyIg) • Pre-B (cy Ig) • B-cell (sIg) 3% (FAB L3, CMYC gene trans) Mature B-cell phenotype no longer confers a poor prognosis
Prognostic Variables • Leukemic Cell Characteristics: • Immunophenotype: • T- Cell ALL : CD2, CD7, CD5, CD3 Males, Older Age, High WBC, Mediastinal mass 12 % of ALL T-cell phenotype no longer confers a poor prognosis
Prognostic Variables • Cytogenetics: • Favorable Prognosis • High Hyperdiploidy: 51 -65 chromosomes/cell or DNA index > 1.16 • Trisomies 4, 10, 17 • TEL/AML1 t(12;21) • Poor Prognosis • Hypoploidy: < 44 chromosomes • Philadelphia chromosome • T(4;11) with MLL-AF4 fusion
Prognostic Variables • Response to Initial Therapy: • Day 7 and Day 14 BM responses Rapid response is favorable Current COG protocols • Peripheral blood response to steroids Day 7 (blasts< 1000/ul) GR is favorable BFM protocols
EARLY RESPONSE TO THERAPY • Rapidity of response to initial chemotherapy is a significant predictor of long-term outcome
Treatment • Induction of Remission (4 -6 weeks) • Consolidation ( 4 -8 weeks) • Interim Maintenance (8 weeks) • Delayed Intensification (8 weeks) • Maintenance (2 -3 years)
Treatment • Induction of Remission Standard or Low Risk Dexamethasone Vincristine L Asparaginase High Risk Dexamethasone/Prednisone Vincristine L Asparaginase Anthracyclines (Daunomycin)
Treatment • Induction of Remission Dexamethasone Low Risk Less CNS and BM relapses Better EFS Use in Adolescents Aseptic Necrosis Use in High Risk Infections
Treatment • Consolidation: • Intensified CNS therapy • Delayed Intensification: • improves outcome • Anthracyclines, Cyclophosphamide
Treatment • Maintenance Therapy: • Daily oral 6MP and weekly oral MTX • Severe hematopoietic toxicity with Thiopurine S Methyl Tranferase deficiency • CNS prophylactic therapy
Treatment Maintenance Therapy: • VCR + Prednisone/ Dexamethasone Pulses • VCR/Prednisone pulses improved EFS • Dexamethasone in 1-9 yr SR patients showed fewer CNS relapses and improved EFS compared to Prednisone • Use of Dexamethasone in Adolescents: Risk of Aseptic Necrosis and bone fractures
Treatment • T-cell ALL: Intensified chemotherapy protocols Pilot trials with ARA-G • Infant ALL: Intensive chemotherapy protocols • Philadelphia +ve ALL: BMT from matched related or MUD Imatinib
Relapsed ALL • Timing of Relapse: Early Relapse: Survival < 10-20% [ Relapse on therapy or 6 months off ] Late Relapse: Survival 30-40% (chemotherapy) [ Relapse 12 months off therapy] T-cell ALL: Survival < 20%
Treatment of Relapsed ALL • Bone Marrow Transplantation: Early Relapse High Tumor Load (>10,000 blasts/ul) • Chemotherapy
Conclusions • ALL is the commonest leukemia of childhood • Minimal evaluation should include a good H&P, peripheral smear and bone marrow exam • Simple treatment protocols utilizing common agents used for ALL treatment should be used initially • Treatment modifications should be based on institutional experience and results