Download

1 / 11
200 likes | 1.29k Views
Miscarriage. Manaia Health PHO 19 March 2014. Definition. A miscarriage is a pregnancy loss due to natural causes before 20 weeks gestation. Causes of Miscarriage. Embryo/fetal Causes

E N D
Miscarriage Manaia Health PHO 19 March 2014
Definition • A miscarriage is a pregnancy loss due to natural causes before 20 weeks gestation
Causes of Miscarriage • Embryo/fetal Causes • The embryo, fetus or placenta are abnormal; there is early fetal demise followed by spontaneous expulsion of the pregnancy • Maternal Causes • The pregnancy is normal, but there is a maternal medical disorder or complication causing fetal demise and/or expulsion of the pregnancy
Embryo/fetal Causes of Miscarriage • Mostly sporadic genetic abnormalities • Usually first trimester • Occasionally chromosomal problems will lead to fetal demise in the 2nd trimester (trisomy 21, 18, 13, triploidy, 45XO) • Sometimes a subchorionic haematoma may lead to 2nd trimester miscarriage, probably due to ascending infection
The Natural History of Early Fetal Demise • Early embryonic or fetal demise typically occurs at 4-8 weeks gestation • Trophoblast usually continues to function for 2-6 weeks and symptoms of pregnancy persist • Eventually trophoblast function declines and the uterus expels the pregnancy with a variable amount of pain and vaginal bleeding
Clinical Presentation and Scan Findings • Women with early pregnancy bleeding may have a viable or a non-viable pregnancy • bhCG measurements do not distinguish viable from non-viable pregnancies • If a viable pregnancy is seen on scan miscarriage is very unlikely • If a non-viable pregnancy is confirmed on scan it is likely that fetal demise occurred several weeks prior to presentation
Routine Early Pregnancy Scans • If a routine early pregnancy scan fails to confirm a viable pregnancy: • This may be early fetal demise or • The scan may have been done too early • It is not possible to confirm early fetal demise if: • The mean gestational sac diameter is <25mm or • The CRL is <7mm • If in doubt it is usually best to manage expectantly and rescan after at least 1 week. bhCG doesn’t help!
Management of Miscarriage • After fetal demise most pregnancies will miscarry completely. Interventions speed up the process but do not reduce average blood loss • Interventions available: • Medical – misoprostol (if already signs of mc) +/- mifepristone (if no sign of MC) • Surgical – dilatation & suction evacuation; this is associated with a higher risk of infection and a risk of uterine perforation
Maternal Problems Causing Miscarriage • These only cause a small minority of miscarriages. • 1st trimester – anti-phospholipid syndrome, viral infections • 2nd trimester – uterine abnormalities, cervical incompetence, fibroids
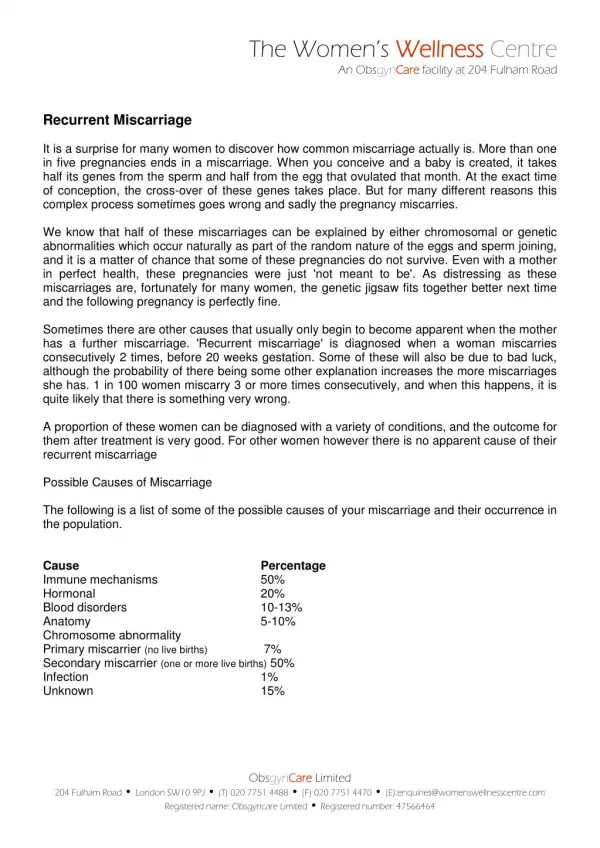
Recurrent Miscarriage • Definition: • 3 consecutive spontaneous 1st trimester losses • 2 consecutive spontaneous 2nd trimester losses • Affects about 1% of women trying to conceive • An underlying cause is only found in a minority • If there is an underlying cause it must be a parental abnormality
Causes of Recurrent Miscarriage • Maternal medical problems • Antiphospholipid syndrome • Balanced chromosomal translocation • Abnormal uterus (congenital or acquired) – cone biopsy, repeated or late TOP, childbirth trauma • If no cause found high chance of subsequent successful pregnancy. • Avoid empirical treatment; however reassurance scans in the 1st trimester increase the likelihood of a successful pregnancy