Download
1 / 26
280 likes | 955 Views
The Management of Miscarriage. Max Brinsmead PhD FRANZCOG March 2013. Resources. RCOG Greentop Guidelines “The Management of Early Pregnancy Loss” October 2006 Updated September 2011 MWB Guidelines for the conduct of an Early Pregnancy Assessment Service 2006. Preamble.

E N D
The Management of Miscarriage Max Brinsmead PhD FRANZCOG March 2013
Resources • RCOG Greentop Guidelines “The Management of Early Pregnancy Loss” October 2006 • Updated September 2011 • MWB Guidelines for the conduct of an Early Pregnancy Assessment Service 2006
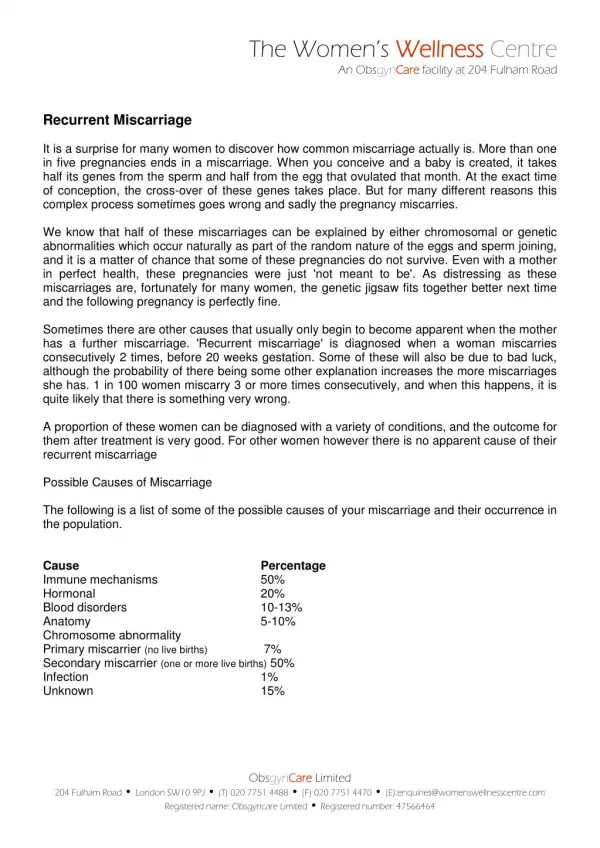
Preamble • Spontaneous abortion occurs for 10 - 20% of clinical pregnancies • Traditional management was “D&C” for 50 yrs • More recently conservative and medical management have been tested by RCT • They have been found to have: • Fewer risks and complications • Less cost • Greater patient satisfaction
But non-surgical management of miscarriage requires... A systematic approach to assessment Close follow up Timely intervention when indicated or requested In many hospitals this is provided by an “Early Pregnancy Assessment Unit”
Traditional approach to miscarriage • Examination of the genital tract for signs of pregnancy and miscarriage • Classified as: • Threatened = No POC passed, cervix closed & uterus enlarged • Inevitable = No POC passed but cervix open & uterus enlarged • Incomplete = POC passes & cervix open • Complete = POC passed & cervix closed • Missed = Pregnancy failure & cervix closed • But high resolution ultrasound has rendered this classification obsolete
Contemporary Classification of Miscarriage • Requires history, examination, ultrasound +/- quantitative measure of beta HCG • Classify miscarriage as: • Threatened = PV bleeding but intrauterine FH seen • Incomplete = POC passed but significant POC remaining • Complete = POC passed and uterus is empty • Early Pregnancy Failure = No POC passed but ultrasound evidence of failed pregnancy • Note that this classification avoids the use of the confusing term “missed abortion” and the unfortunately named “blighted ovum”
And there is one further important category • Undiagnosed Early Pregnancy Problem • That is pain and/or PV bleeding but… • US not yet performed • US unlikely to be helpful because • HCG <1500 IU/L and/or dates <5.5 weeks amenorrhoea • Or US cannot confirm the presence of an intrauterine pregnancy
Because ectopic pregnancy is.... • A common condition • 1:50 pregnancies • Can be fatal if misdiagnosed • So think of every early pregnancy as… • ECTOPIC until proven otherwise
And always remember... • Heterotopic Pregnancy • That is one in the uterus plus an ectopic • Quite rare unless the patient has had assisted conception • IVF with multiple embryos transferred • But difficult to diagnose if ultrasound evidence of intrauterine pregnancy is taken to exclude ectopic pregnnacy
A worrying trend When a patient is thought to be pregnant then the doctor or nurse arranges a quantified beta HCG and an ultrasound scan No history, no exam just tests! But there is no substitute for a careful history Because it is essential for the interpretation of some ultrasound findings So please don’t just rely on the radiologist’s report!
Some tips and cues in taking a history • Is this a planned pregnancy? • Dates are more reliable if planned • Also helps to gauge the patient’s psyche • What method of family planning did you use prior to that? • Beware of COC and Depot • When was your last pregnancy (baby)? • For how long did you breast feed? • Has the patient had time to establish a cycle?
Some tips and cues in history taking 2 • What was the first day of your last period? • Not the date of the first missed period • Provide suggestions e.g. “before or after Xmas” • Keep trying for the best estimate of a date • Was that a normal period? • Normal in timing, duration and amount • Do you have regular periods? • What do you mean by regular? • What do you mean by irregular, how early, how late?
Some tips and cues in history taking 3 • When did you first think you might be pregnant? • Has your pregnancy been confirmed? • How, when and by whom? • Urine pregnant test becomes positive at the time of the missed period (if it is a normal pregnancy) • Have you had any scans? • When did that doctor/midwife suggest your baby might be due? • Do you still feel pregnant?
Do all patients require vaginal exam? • Most patients deserve a pulse rate, BP measure and abdominal palpation • Vaginal exam is required when... • Ultrasound is not readily available • There has been substantial bleeding • If the patient is hypotensive • It may be corrected by clearing the cervix • The patient reports passage of tissue • Clear the cervix • Collect any tissue to confirm the pregnancy • There is doubt about the source of bleeding • There is the possibility of ectopic pregnancy • But please be very gentle
Who (or when) to refer for early pregnancy assessment • Any vaginal bleeding • Some 15 - 30% of women will have first trimester bleeding or spotting • And 50% of patients with vaginal bleeding will have a failed early pregnancy • Pelvic pain is not responding to simple measures • High risk patient • History of recurrent miscarriage • High risk of ectopic esp. previous ectopic • Advanced maternal age • Patient anxiety
Criteria for the ultrasound diagnosis of Early Pregnancy Failure • Must be a vaginal scan in all cases • Mean gestational sac size > 25 mm and no fetal heart motion detected • Embryo >7 mm seen but no fetal heart motion detected • If in doubt... • Tell the patient • Seek a second opinion or • Rescan in 7 – 14 days
Pathology tests required • Blood group (if not known) and BGA • HB or FBC • Quantified beta HCG • But this is pointless if sent for immediate scan • Urine PCR for Chlamydia in high risk woman • Age < 25 yrs • Relationship < 6 months or multiple partners • HVS and Blood C/S if septic • Routine antenatal tests if the pregnancy is continuing • HIV in all patients is desirable
Options for the management of early pregnancy failure Surgical evacuation of the uterus Medical evacuation of the uterus Wait and see
Surgical management is recommended when... • The patient is febrile (>37.50 C) • After appropriate antimicrobial management • The cervix is closed and the sac > 5cm diam • The patient has miscarried twice before • Collect tissue for chromosomes • The patient or your health facilities are incapable of appropriate follow up
Medical management is recommended when • There are fetal parts >14 weeks in size • Surgical evacuation is unsafe • The pregnancy is >10 weeks in size, the patient elects D&C & cervix is closed • Use Misoprostol 400 mcg to ripen the cervix 3-4 hrs prior to dilatation • There is DIC or some other contraindication to surgery or anaesthesia
Medical management of early pregnancy failure or incomplete miscarriage • 2 x 200 mcg Misoprostol into the posterior fornix • Repeat in 4-6 hrs if required • Must scan or evaluate clinically to confirm that evacuation is complete • In general echogenic material >16 mm in AP diameter is required for the US diagnosis of retained products of conception • (better termed incomplete miscarriage)
Conservative management of early pregnancy failure or incomplete miscarriage Repeat clinical and USS evaluation after 3 days Then 7 days and weekly Must telephone or come in at any hour if pain or bleeding is unacceptable or fever occurs
Possible outcomes from nonsurgical management Several weeks of follow up may be required 20 - 50% of patients request or require curette Some resorb the trophoblastic tissue with little or no bleeding Others bleed for weeks
Other aspects of management • Anti-D is required for EP bleeding if Rh Neg • Send all tissue for histology • Provide or arrange psychological support • Patients want an explanation for the loss • And advice about the future • Or contraceptive advice • Offer referral to GP, counsellor or a Support Group
The Emergency Department Management of an early pregnancy problem • IV Fluids are required only for hypovolaemia • Ultrasound is not appropriate if: • < 5.5 weeks amenorrhoea • >12 weeks & uterus is palpable because a Doppler by a midwife is diagnostic of fetal viability • The patient is shocked or in pain • For vaginal examination you require: • Some experience • Privacy • A good light • Some assistance • Some instruments to swab the vagina or clear the cervix
Monitoring an early pregnancy problem • Beta HCG <250 iu/L • You can watch and wait • Admit for obs if there is a strong suspicion of ectopic • Repeat quantified beta HCG in 24 hrs • A successful pregnancy will double every 48 - 72 hrs • Beta HCG 500 – 1000 iu/L • As above but laparoscopy required if there are symptoms or signs of ectopic • Beta HCG >3000 iu/L and an empty uterus = Ectopic Pregnancy • Beta HCG 1000 - 3000 iu/L and vaginal ultrasound equivocal • Laparoscopy best if there is any question of ectopic