Download
1 / 41
440 likes | 700 Views
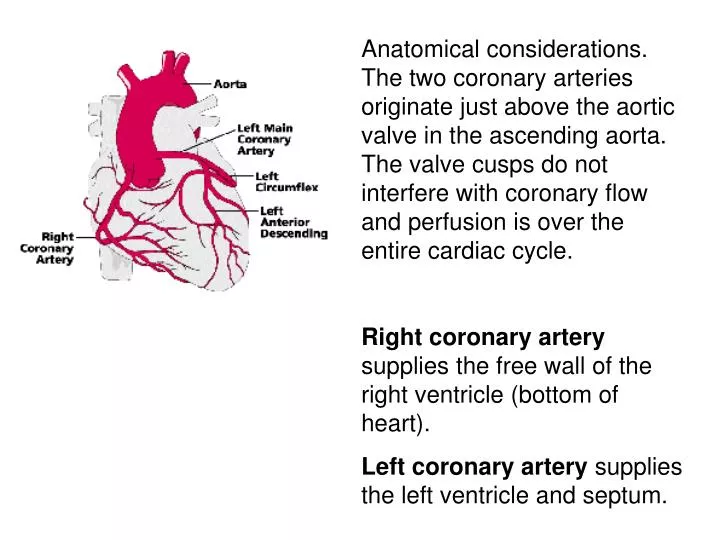
Anatomical considerations. The two coronary arteries originate just above the aortic valve in the ascending aorta. The valve cusps do not interfere with coronary flow and perfusion is over the entire cardiac cycle.

E N D
Anatomical considerations. The two coronary arteries originate just above the aortic valve in the ascending aorta. The valve cusps do not interfere with coronary flow and perfusion is over the entire cardiac cycle. • Right coronary artery supplies the free wall of the right ventricle (bottom of heart). • Left coronary artery supplies the left ventricle and septum.
Coronary blood flow (CBF) Resting ≈ 1 ml/min/gm. About 200 ml/min for a 200 gm human heart. ~5% of the cardiac output. The heart is always in an active hyperemia because the heart is a working muscle.
95% of the oxygen is extracted from the coronary blood on a single passvs. ~ 75% for the rest of the body. Metabolism is primarily by beta oxidation of FFA. Glucose oxidation accounts for only about 15% of metabolism
Notice the reactive hyperemia following the occlusion. Theheart requires a continuous metabolic supply. Only 10 sec of coronary artery occlusion causes a marked drop in contractility. If continued the ventricle will be akinetic in 40-60 seconds Ischemia:inadequate blood flow
During ischemia glycolysis of glycogen and glucose increases and becomes the only energy source but it cannot maintain the heart even when contraction has stopped. Oxygen is the rate-limiting metabolite in ischemia.
Cell death starts at ~20 min after the onset of coronary occlusion and continues over the next 6 hr. Often the occlusion involves only a small branch and the heart will continue to pump blood. If the region can be reperfused quickly the ischemic region can fully recover.
If a large branch is involved the ischemically depressed heart may not be able to pump and cardiovascular collapse may occur (sudden death or the so called “massive heart attack”). CPR is needed to supply enough coronary blood to maintain the contractility so that the heart can pump when defibrillated.
Three Factors Control CBF • Metabolic: Autoregulation • Mechanical • Neural
B C A Autoregulation makes flow independent of pressure. B is on the instantaneous line while C is on the steady-state line hypoxia ATP adenosine + 3Pi
If heart rate slowed, it would be shifted down. Flow Is Intimately Coupled to Myocardial O2 Consumption If heart rate were increased the steady-state line would be shifted up.
Energy requirements = internal + external Pressure External Work Internal Work Ventricular volume Increasing contractility increases oxygen demand
Reducing contractility with a beta blocker would shift the line down. Contractility Affects Coronary Blood Flow Increasing contractility by stimulating the sympathetic nerves would shift the line up.
Metabolites such as adenosine are released when flow does not meet the metabolic demand. These factors then dilate the coronary arteries to increase the flow.
Three Factors Control CBF • Metabolic • Mechanical. With each beat thecontracting heart muscle squeezes the coronary arteries and increases their resistance to flow. • Neural
Left coronary flow during systole is depressed even though the pressure gradient is highest at that time. The effect is less dramatic in the right coronary because the compressive forces in the tissue are much lower in the right ventricle
The compression is the result of blood pressure in the lumen of the ventricle being transmitted through the ventricular wall. As a result compressive stress is equal to ventricular pressure in the subendocardium and falls to near zero at the subepicardium. To compensate the loss of flow during systole the diastolic flow is higher. The average is the same across the wall
Compressive stresses inhibit blood flow through the microcirculation. As a result flow is distributed away from the subendocardium during systole. Autoregulation senses the deficit in flow to the inner layers and dilates blood vessels in that region so the diastolic flow will be higher and compensate the loss during systole. To compensate the loss of flow during systole the diastolic flow is higher. The average is the same across the wall
Autoregulation compensates the loss due to mechanical factors so that flow across the wall is uniform despite the added mechanical impediment to flow in the deep layers
If coronary perfusion pressure is reduced due to arterial narrowing, the arterioles become maximally dilated and flow to the subendocardium can no longer be compensated. Subendocardial ischemia
Counterpulsation inflate the aortic balloon during diastole and deflate it during systole. Lowers peak ventricular pressure (less blood flow need) Raises diastolic aortic pressure (more blood flow supply).
III. Three Factors Control CBF • Mechanical • Metabolic • Neural:The coronary arteries are under very limited neural control
Increased contractility and heart rate causes net secondary dilation due to increased oxygen consumption (metabolic wins over direct neural control of the blood vessels). Sympathetic stimulation Causes a weak Alpha - constriction that is only transient
A reduced coronary sinus PO2 indicates that the coronary flow is not as high as the heart would have liked. (Some residual constriction due to the Error Signal!)
The parasympathetic stimulation has virtually no primary effects because few vagal fibers reach the ventricle (would have dilated the arterioles). A secondary parasympathetic vasoconstriction is caused by autoregulation because reducing the heart rate reduces metabolic demand.
Coronary collaterals: (anastomoses between the coronary arterial branches) Collateral vessels maintain some tissue blood flow after complete occlusion of an arterial branch. This residual blood flow is nutritional and most infarcts are not transmural thanks to collateral flow.
Native collaterals can provide about 10-20% preocclusion flow in humans. That is not enough to prevent infarction. • Gradual occlusion over months as occurs with a developing atherosclerotic plaque causes collateral development. Some patients even have complete occlusion with few symptoms.
Collaterals occur above the arterioles (artery to artery). Thus they supply the entire occluded bed equally. Cells close to the margins of an ischemic zone have no advantage
Acute myocardial infarction: a sudden occlusion of a coronary artery (common heart attack).
Fresh Infarct Healed Infarct
Three factors determine infarct size 1. Sizeof the ischemic zone 2. Level of collateral flow 3. Duration of ischemia
Therapeutic growth of collaterals with VEGF was tested but the results were not promising.
Three factors determine infarct size 1. Sizeof the ischemic zone 2. Level of collateral flow 3. Duration of ischemia
A wavefront of tissue death starts at the endocardium and progresses to epicardium over a 6hr period. Reperfusion can be accomplished with thrombolytic drugs or direct angioplasty and is the primary treatment for these patients Hearts can be made resistant to infarction with salvage-inducing drugs (still experimental)
Angina pectoris Due to narrowing of the coronary arteries Ischemic pain from the heart is usually felt in the chest but may be referred to the arm or jaw. Attacks are often brought on by increased metabolic demand of the heart caused by physical exertion.
Angina pectoris Often treated medically with agents that reduce cardiac demand e.g. beta blockers, calcium antagonists and nitrates.
Percutaneous coronary transluminal angioplasty (PCTA) In selected patients treatment is to dilate the narrowed region with an angioplasty balloon and a wire stent.