Download
1 / 93
960 likes | 1.38k Views
FFR Going Beyond Angiography. By Amr El Nagar. Should this lesion be stented ??. Back to the Basic Coronary Physiology. • Coronary blood flow = 3-5% of C.O. • Resting myocardial O2 demand is extremely high (20 x skeletal O2 demand) • Myocardium extracts maximum O2

E N D
FFR Going Beyond Angiography By Amr El Nagar
Back to the Basic Coronary Physiology • Coronary blood flow = 3-5% of C.O. • Resting myocardial O2 demand is extremely high (20 x skeletal O2 demand) • Myocardium extracts maximum O2 from blood (80% versus 30-40% skeletal muscle) • Myocardium has high capillary density (3000-4000/mm2 versus 500-2000/mm2 skeletal muscle) • Therefore, only way to meet increasing demand is to increase blood flow
Coronary Blood Flow vs Percent Diameter StenosisAutoregulationAutoregulation
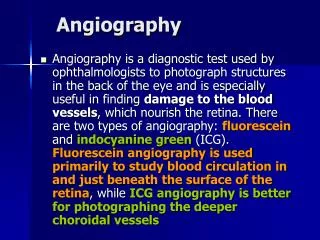
Hyperemia • Hyperemia is a state of myocardial vasculature dilatation • Myocardial bed can be pharmacologically dilated with an agent eg:Adenosine • occurs naturally in the body in small quantities and is produced during exercise to assist in the dilatation of the myocardial bed.
FFR • What ?????????????? • Why??????????????? • How?????????????? • When????????????? • $$$$$$$$$$$$$$$$
What is FFR? It is aRatiobetween Maximum flow down a vessel in the presence of a stenosis… …and maximum flow in the hypothetical absence of the stenosis
Derivation of FFR • FFR = Coronary Flow(Stenosis) Coronary Flow (Normal) • Coronary Flow = Pressure Resistance • at maximal hyperemia Coronary Flow ≈Pressure So, FFR = Coronary Pressure(Stenosis) Coronary Pressure (Normal)
FFR threshold for ischemia No ischemia Yes ischemia FFR 1.00 0.75 0.00 FFR < 0.75 inducible ischemia (spec. 100 % ) FFR > 0.75 no inducible ischemia (sens. 90 % ) Pijls, De Bruyne et al, NEJM 1996
Why FFR(is it superior)???? *Stenting of non-ischemic stenoses has no benefit compared to medical treatment only. *Stenting of ischemia-related stenoses improves symptoms and outcome. *In multivessel coronary disease (MVD), identifying which stenoses cause ischemia is difficult. *Non-invasive tests are often unreliable in MVD and coronary angiography often results in both under or overestimation of functional stenosis severity.
Limitations of Anatomic Techniques: - Underestimates diffuse disease - Large Intra- and inter-observer variability - Not designed to assesses physiologic lesion significance
Limitations of Non-Invasive StudiesSPECT Imaging - SPECT imaging 70% sensitivity for single vessel disease - SPECT imaging has 85-90% sensitivity for detecting disease in patients with MVD, but only 50% sensitivity for detecting MVD ischemia pattern
But FFR!!!! • FFR is not influenced by changes in blood pressure, • heart rate, or contractility • FFR has a unique normal value of 1.0 in every patient • and every coronary artery • FFR incorporates the contribution of collateral flow • to myocardial perfusion
Pressure Wire Tip • Guide wire - 0.014 • straight or ‘J’ tip • pressure sensor - 3 cm proximal to the end of the wire Pressure sensor
Equipments RADI ANALYZER PRESSURE WIRE
Myocardium Aorta coronary artery 100 0 Qnormal Pa Pd Max. hyperemia Normal perfusion pressure 100 0 Pd Pa Qstenosis Stenotic perfusion pressure Qstenosis Stenotic perfusion press. Pd FFR = = = Qnormal Normal perfusion press. Pa
blood pressure distal to the lesion being assessed - Pressure distal (Pd) • conventional pressure transducer - measures arterial/aortic pressure - Pressure arterial (Pa)
mean pressures of Pd and Pa are used • assuming there is no lesion present = no difference in pressure • The difference between these two pressures taken at rest determines if there is a resting gradient across a lesion • Gradient calculation = Pd/Pa.
no lesion, the pressures will be the same and therefore the gradient value will be 1 • e.g. Pa = 150 mmHg Pd = 150mmHg • So, Pd/Pa = 1
Dilation of micro-vasculature increases oxygen demand • a flow limiting lesion will cause the blood pressure distal to the lesion to fall • FFR will fall • The extent of this reduction gives an indication as to the degree of flow limitation and hence degree of severity of stenosis
Technical: • loose connection • leak in guide connections • improper zero • Inadequate hyperemia Anatomic/Theoretical: • Ostial, diffuse disease • microvascular disease • Extreme tortuosity • Serial lesions Mechanical/Hemodynamic: • Guide catheter obstruction • Low drug delivery
Insufficient Hyperemia IV Adenosine:- • Check infusion, pump system and lines • Infuse through central vein • Avoid Valsalva maneuver during infusion For Intracoronary route:- • Guiding catheter failure to seat • flow obstruction-incorrect dose mix or dilution • incorrect dose mix or dilution
Reasons of Non-ischemic FFR Despite an Apparently Tight Stenosis Physiologic explanations: • Stenosis hemodynamically nonsignificant despite angiographic appearance • Small perfusion territory, old MI, little viable tissue, small vessel • Abundant collaterals • Severe microvascular disease (rarely affecting FFR) Interpretable explanations: • Other culprit lesion, diffuse disease not focal stenosis • Chest pain of noncardiac origin
Technical explanations: • Insufficient hyperemia • Guiding catheter related pitfall (deep engagement, small ostium,sideholes) • Electrical drift Actual false negative FFR: • Acute phase of ST elevation myocardial infarction • Severe left ventricular hypertrophy • Exercise-induced spasm
When FFR???(value) • Borderline lesions • Evaluation of PCI FFR after coronary intervention should preferably be higher than 0.90
Multicenter registry Europe-USA-Asia750 pat. post-STENT FFR % death, infarction, or re-intervention at 6 mnths. 40% 37% After stenting:Inverse correlation between FFR and event rate. 28% 30% 19% 20% 7% 10% 4% 0% 0.76-0.80 0.81-0.85 0.86-0.90 0.91-0.95 0.96-1.00 Post-STENT FFR
How does FFR works in complex coronary disease? difficult anatomy, poorly visible lesions, overlap multiple stenoses within one artery diffuse disease left main disease multivessel disease
Male, 67, stable angina, positive exercise test LCX D 2 RCA LAD D 1 2 intermediate stenoses mid RCA Complex lesion proximal LAD
LAD, hyperemia Pa Pa 100 Pd Pd FFR = 92/98 = 0.94 0
DIAG 2, hyperemia Pa Pa 100 Pd Pd FFR = 87/97 = 0.89 0
DIAG 1, hyperemia Pa Pa Pd 100 Pd FFR = 87/96 = 0.90 0
RCA, hyperemia Pa 100 Pd 0 FFR = 38/92 = 0.41
After balloon inflation 3.0 balloon 12 atm Pa 100 Pd FFR = 55/82 = 0.67 0
Stent 3.5 mm(mid-RCA) Pa 100 Pd FFR = 76/95 = 0.80 0
Pressure drop Pull back pressure wire
Additional Stent 3.5 mm (prox-RCA)
Stent 3.5 mm(mid-RCA) + Stent 3.5 mm(prox-RCA) Pa 100 Pd FFR = 88/94 = 0.94 0
In this patient with complex coronary artery disease, • coronary pressure measurement: • confirmed the appropriateness of stenting the RCA • while avoiding a riskful intervention of the LAD • or bypass surgery • Selected the correct spots in the RCA where to stent • evaluated the result of stenting.
How does FFR works in complex coronary disease? difficult anatomy, poorly visible lesions, overlap multiple stenoses within one artery diffuse disease left main disease multi vessel disease
A B