Download

1 / 21
210 likes | 383 Views
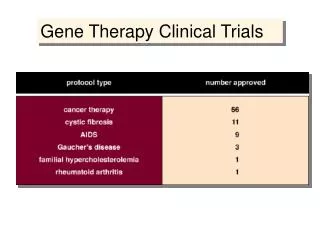
Design of Clinical Trials of Antibiotic Therapy for Acute Otitis Media. Colin D. Marchant, M.D. Boston University School of Medicine and Tufts University School of Medicine. FDA Anti-Infective Drugs Advisory Committee Meeting, July 11, 2002. 17/253 (7%). P < 0.001. 15/40 (38%).

E N D
Design of Clinical Trials of Antibiotic Therapy for Acute Otitis Media Colin D. Marchant, M.D. Boston University School of Medicine and Tufts University School of Medicine FDA Anti-Infective Drugs Advisory Committee Meeting, July 11, 2002
17/253 (7%) P < 0.001 15/40 (38%) 2/66 (3%) P < 0.001 21/57 (37%) Culture-positive on day 3-7 Culture-negative on day 3-7 Correlation Between Clinical and Bacteriological Outcome in Acute Otitis Media Clinical Failure Clinical Success Carlin et al J Pediatr 118:178-83, 1991 Dagan et al Pediatr Infect Dis J 17:776-82, 1998
The Pollyanna PhenomenonMeasuring the Efficacy of Anti-bacterial Drugs in Acute Otitis Media Clinical Efficacy Bacteriologic Efficacy Clinical Efficacy in Bacterial AOM Drugs appear, and are equal Excellent drugs appear worse than they really are Poor drugs look better than they really are Placebo Marchant CD, et al J Pediatr 1992;120:72
Sample Sizes Required to Detect Differences Between Antibacterial Drugs for Acute Otitis Media (AOM): Comparison of Bacteriologic Versus Clinical Outcomes in a Trial of 2 Drugs With Varying Bacteriologic Efficacy (Half the patients would be in each arm of a study) Measuring the comparative efficacy of antibacterial agents for acute otitis media: The “Pollyanna Phenomenon.” Colin D. Marchant, Susan A. Carlin, Candice E. Johnson, and Paul A. Shurin. J Pediatrics 1992;120: 72-77.
Clinical Impact of Drug Efficacy Based on Marchant et al J. Pediatr 1992;120:72
Clinical Impact of Drug Efficacy Based on Marchant et al J. Pediatr 1992;120:72
Design Issues All are important, but in relative order of importance: Otitis Media specific: • Sample size • Outcome measures • Patient selection – low/high risk • Diagnostic criteria at entry General: randomized, double-blind, compliance, etc.
Four Trial Designs • “Double Tap” • “Tap at Entry and Tap of Clinical Failures” • “Tap at Entry with Clinical Outcome” • Clinical Criteria for Entry and Outcome
Parameters Used in Sample Size Calculations • Significance level = 0.05 • Power = 0.90 • Inverse sine method • All sample sizes are for a 2-limbed trial with half of subjects in each limb
Sample Sizes and # of Tympanocenteses (Taps) Various Study DesignsGood Drug (90%) vs. Placebo (30%) Based on data of Marchant et al J. Pediatr 1992;120:72 and Dagan et al Pediatr Infect Dis J 1998;17:776.
Sample Sizes and # of Tympanocenteses (Taps) Various Study DesignsGood Drug (90%) vs. Poor Drug (50%) Based on data of Marchant et al J. Pediatr 1992;120:72 and Dagan et al Pediatr Infect Dis J 1998;17:776.
Sample Sizes and # of Tympanocenteses (Taps) Various Study DesignsGood Drug (90%) vs. Fair Drug (70%) Based on data of Marchant et al J. Pediatr 1992;120:72 and Dagan et al Pediatr Infect Dis J 1998;17:776.
Sample Size for Measuring Efficacy of Antibiotics in Acute Otitis Media • Depends on the outcome selected • Depends on population studied • Minimum standard: Large enough to demonstrate that a new antibiotic is better than no antibiotic – otherwise efficacy has not been measured • Adequate standard: Should exclude a 20% difference in bacteriologic efficacy between antibiotics – ensure that no more than 40,000 children per million children treated will remain symptomatic because of unmeasured inferiority
Recommended Guidance for IndustrySample Size • Response rates (eradication, clinical, etc) should be based on data from clinical trials, not assumption or expert opinion • Trial size must be large enough to demonstrate that a drug is a least better than a placebo. • The difference between two drugs should be a clinically important one, such as persistent symptoms at a rate of 40,000 per million prescriptions, i.e. a 20% difference in bacteriologic efficacy • Should also consider the power of sub-group analyses, e.g. organism specific response rates
Outcomes for Measuring the Efficacy of Antibiotic Therapy in Acute Otitis Media • Directly meaningful, or validated against meaningful outcomes • Objective or at least reproducible • Sensitive (are affected by antibiotic therapy) • Timely – measured at a time point when antibiotic therapy has an effect • Supported by evidence (not assumption)
Outcomes in Clinical Trials of Antibiotic Therapy in Acute Otitis Media Information increases Eradication by MIC Pathogen eradication rates, Correlations with PK/PD, etc. 1. “Double Tap” 2. “Tap and Tap of Clinical Failures” 3. “Tap at entry and Clinical Outcome” 4. Clinical Outcome Sample Size Decreases
Recommended Guidance for IndustryTrial Design - Tympanocentesis • “Double tap” studies are preferred - have been validated, provide more information, and require the smallest sample size, and the fewest number of taps (among studies with taps) • “Tap and Tap of Clinical Failures” is an alternative that if large enough will provide useful information • If clinical outcomes other than symptomatic response are to be used as outcomes, they should be validated
Recommended Guidance for IndustryPopulation Selection/Enrichment • Trials should include “enriched’ populations: The young, treatment failure, prior antibiotic therapy, day care, etc are the most challenging cases and clinicians need to know whether antibiotics are efficacious in these patients. These patients should be included, not excluded from clinical trials
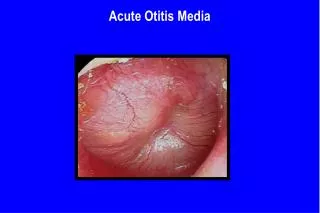
Recommended Guidance for IndustryDiagnostic Criteria • Symptoms: should have at least one of: earache, irritability, fever • Otoscopic exam: should have at least one opaque, bulging eardrum with reduced mobility • A trial site should isolate pathogens from at least 70% of cases at entry
Ethical Issues • Is it ethical to license, market and prescribe drugs without knowing that they are efficacious (pass the tap water standard)? • Is it ethical to perform drug trials in humans that will not yield scientifically valid data? • Is it ethical to perform tympanocentesis? • Is it ethical to perform double tympanocentesis studies?
Do the benefits outweigh the risks? • Tympanocentesis is briefly painful but not permanently harmful • The benefits of the knowledge gained outweigh the risks • Still, there is a need for research into the effectiveness of various methods of systemic and topical analgesia/anesthesia for tympanocentesis should be performed (industry should sponsor such studies).