Download
1 / 15
150 likes | 315 Views
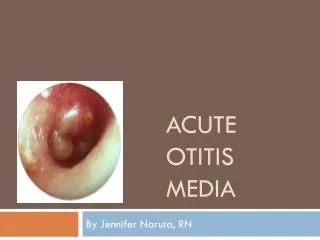
Clinical Trials of Acute Otitis Media. John Alexander, M.D., M.P.H. Anti-Infective Drugs Advisory Committee November 7, 2001. History. Kefauver-Harris Amendments (1962) Clinical Evaluation of Anti-Infective Drugs (1977)

E N D
Clinical Trials of Acute Otitis Media John Alexander, M.D., M.P.H. Anti-Infective Drugs Advisory Committee November 7, 2001
History • Kefauver-Harris Amendments (1962) • Clinical Evaluation of Anti-Infective Drugs (1977) • “It is necessary to confirm the presence of exudate in the middle ear by pneumotoscopy and needle aspiration to obtain fluid for culture.” • “In the absence of culture of middle ear fluid, no specific claim can be made regarding the effectiveness of any anti-infective drug.”
History • Points to Consider Document (1992) • “Statistically adequate and well-controlled multi-center trial … establishing equivalence or superiority to an approved product” • “Open study … using tympanocentesis … at baseline to establish microbiologic etiology” • At least 25 patients with S. pneumoniae • At least 25 patients with H. influenzae • At least 15 patients with M. catarrhalis • FDA/IDSA (CID Supplement Nov. 1992) • Draft Guidance for Industry Documents (1998)
Draft AOM Guidance • Two Studies recommended: • “A statistically adequate and well-controlled multi-center trial … establishing safety and effectiveness” • “Another trial … using tympanocentesis … at baseline to establish microbiologic etiology” • At least 25 patients with S. pneumoniae • At least 25 patients with H. influenzae • At least 15 patients with M. catarrhalis
Draft AOM Guidance • For the first trial (clinical-only study): • Ordinarily should not enroll children <6 months • Rigid case definitions • Baseline tympanocentesis need not be performed • “Tympanocentesis of patients judged to be therapeutic failures is strongly encouraged to document potential specific bacterial pathogens not adequately treated in the trial.”
Draft AOM Guidance • For the second trial (Micro Study): • “Post-therapy tympanocentesis is encouraged [in] patients judged to be therapeutic failures” • 2 investigators in geographically diverse regions • Acceptable clinical and microbiologic effectiveness against all three microorganisms • Resistance and S. pneumoniae, 25 patients may be insufficient
Draft AOM Guidance • Study Visits • Entry Visit • On Therapy (3-5 days): Strongly recommended • End-of-Treatment: Optional • Test-of-Cure: 2-4 weeks after entry • Late Post-Treatment Follow-Up: Optional
AC Meetings on AOM • Guidance for Industry (March 1997) • Ceftriaxone for AOM (Nov. 1997) • Guidance Revisions (July 1998) • Augmentin ES-600 for AOM (Jan. 2001)
AC Meetings on AOM • Spring 1997 - Presentation of Guidance • Baseline clinical findings • Timing of the TOC visit • Number of S. pneumoniae isolates in light of increasing resistance • Follow-up of middle ear effusion out to 30 days
AC Meetings on AOM • Fall 1997: Ceftriaxone for AOM • Discussion focused on product • Comments on resistant S. pneumoniae • Comments related to study design
AC Meetings on AOM • 1998 - Guidance revisited • Presentation of changes based on Spring ‘97 AC • Letter from CDC to FDA: “Since clinical-only studies would need to be prohibitively large to detect a difference if one truly existed between two drugs … smaller bacteriologically-driven study would be more effective” • Industry response during the AC meeting
AC Meetings on AOM • Jan. 2001 - Augmentin ES-600 for AOM • Discussion focused on product • Timing for the test-of-cure visit • Assessment of bacteriology in clinical failures
AC Meetings on AOM • Nov. 2001 - Zithromax for AOM • Discussion focused on product • Clinical trial design
Issues for Discussion • Should clinical-only trials continue or should all enrolled patients have a tympanocentesis at baseline? • Should non-comparative microbiology studies continue?
Issues for Discussion • Should guidance incorporate stratification by age (< 2 years)? If so, what proportion of patients should be under the age of 2 years? • In your discussion, please comment on the merits of studies with clinical information only, studies with tympanocentesis, ideal timing of clinical assessments (end-of-therapy v. later follow-up), and alternative study designs (comparative trials with microbiology, double-tap studies, placebo-controlled studies with early escape).