Download
1 / 32
330 likes | 905 Views
Prediction of Type 1 Diabetes (T1DM) & related Autoimmune Diseases (AD). Marco Songini, MD Diabetes Unit Azienda Ospedaliera Brotzu Cagliari (Italy) .

E N D
Prediction of Type 1 Diabetes (T1DM) & related Autoimmune Diseases (AD) Marco Songini, MD Diabetes Unit Azienda Ospedaliera Brotzu Cagliari (Italy)
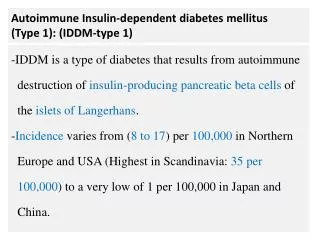
Type 1 diabetes develops from the interaction between susceptibility genes and enviromental determinants. The major genetic susceptibility to type 1 diabetes is conferred by markers from HLA locus, but other genes are involved. The non genetic contribution to the disease (i.e. nutritional factors and infective agents) is even less wll-defined. This may imply aetiological heterogeneity in patients so that particular combinations of genetic susceptibility factors require exposure to specific non-genetic factors in order to initiate the disease developing process in type 1 diabetes. It is well known that immune markers (ICA, GADA, IA2, IAA) appear many years before clinical onset of type 1 diabetes. These “windows” offers the chance to pinpoint subjects at risk eventually suitable to preventive therapies. At present, intervention trials are recommended in the small subset of the population at high risk identified by genetic and immune markers.
Complementary strategies in the prediction of T1DM Strategy 1 AIM: TEST INTERVENTION STRATEGIES High specificity/ low sensitivity families immune markers high risk subgroup Strategy 2 AIM: REDUCE INCIDENCE OF IDDM Low specificity/ high sensitivity general population genetic + immune markers moderate risk subgroup Bingley, E. Bonifacio & E. Gale;Diabetes, vol. 42, feb. 1993
Preventive strategies for T1DM (1) Selective immunosuppression, using depleting or nondepleting monoclonal antibodies to lymphocyte cell surface molecules such as CD3, CD4, CD8, T cell receptor and major histocompatibility complex (MHC) antigens, or blocking peptides to T cell receptors Immunostimulation by viruses, cytokines, calcitriol, concanavalin A, bacille Calmette-Guèrin (BCG), Freund’s adjuvant or tranfusion of deficient lymphocyte subsets B-Cell rest by suppressive therapy with insulin E. Bosi & G.F. Bottazzo; Clin. Immunother. 3 (2) 1995
Preventive strategies for T1DM (2) Protection from oxygen radical-mediated and nitric oxide-mediated damage by nicotinamide, deferoxamine (desferrioxamine) and aminoguanidine Environmental intervention by manipulation of temperature, diet (gluten free) and hormonal milieu Induction of tolerance to B-cells by bone marrow transplantation, lymphocyte transfusion, intrathymic islet transplantation, neonatal B-cell stimulation and administration (intravenous, intrathymic, intraperitoneal or oral) of putative B-cell autoantigens such as insulin or glutamic acid decarboxylase E. Bosi & G.F. Bottazzo; Clin. Immunother. 3 (2) 1995
Tests to predict T1 DM & AD Autoantibodies: ICA, GADA, IA2-A, IAA, AD-Abs HLA-phenotype:DR3/DR4 (DQ2/DQ8), AD phenos HLA-genotype:Eterodimers 57Non Asp/53Arg DQ beta/DQ Alfa, AD genos ? Cell mediated markers: Alteration of lymphocyte subsets CD4/CD8, etc.
Immunological markers for T1DM ICA Islet Cell Abs Indirect immunofluorescence on human pancreatic cryosections Risk at 10 yrs FH+ >10 JDFU 41% >80 JDFU 80% Risk at 5 yrs FH+ 44% IAA Insulin AutoAbs In Children first antibodies to appear R.I.A. Risk at 10 yrs ICA + IAA 81%
Immunological markers for T1DM IA2-A Protein Tyrosin Phosphatase AutoAbs More common among children High specificity low sensitivity R.I.A. GADA Glutamic Acid Decarboxilase AutoAbs High sensitivity low specificity More common among adults R.I.A.
Immunological markers for T1DM Combined markers in FH+ Positivity for 3 or 4 antibodies yelds a risk of 88-100% to become diabetic in 10 years The best association of autoantibodies is: GADA + IA2-A GADA + IA2-A + IAA in young children Pastore MR et al Diabetes Care 1998, 9; 1445-50 We are able to assay GADA + IA2-A on blood spots E. Bosi, E. Bonifacio et al . Diabetes Care - March 1999
Background The preclinical stage of type 1 diabetes and related AD can last even many years These “windows” offers the chance to pinpoint subjects at risk eventually suitable to preventive therapies
Genetic markers for T1DM HLA typing predisposing: HLA DR3-DQ2, DR4-DQ8 protective: HLA DR2-DQ6 Lernmark A Diabetes Metabolism Rev 1998, 14,3-29
Genetic markers for T1DM HLA Molecular biology of DQ chains of class second DQ A301, DQ B302, DQ B501 Alleles: 99% of diabetic patients 50% of normal people Lernmark A Diabetes Metabolism Rev 1998, 14,3-29 DQ B602 is fully protective for T1DM Gianani R et al. J Autoimmunity 1996, 9; 423-425
Genetic markers for T1DM (1) References l Locus s % IDDM1 2,6 35 Davies (1994) 6p21 11p21 IDDM2 1,29 9,4 Davies (1994), Bennet (1995) - - IDDM3 15q Field (1994) IDDM4 1,07 2,5 11q13 Hashimoto (1994), Davies (1994) Davies (1994) IDDM5 1,16 5,5 6q25 3,5 1,1 Meriman (unpub.), Davies (1994) IDDM6 18q Owerbach and Gabbay (1995) IDDM7 1,13 4,5 2q31 Davies (1994), Copeman (1994), 1,42 IDDM8 6q27 12,9 Luo (1995), Davies (1996)
Genetic markers for T1DM (2) l References Locus % s 3q21-q25 1,26 IDDM9 8,5 Reed and Todd (unpubl.) Gough and Todd (unpubl.) 1,45 13,7 IDDM10 10p11.2-q11.2 Davies, Hashimoto (1994) 95.5 TOT. 14 GCK Rowe (1995) 7p Field (1996) 14q24.3-q31 IDDM11 2q33 IDDM12 (CTLA-4) Nistico (1996) 2q34 IDDM13 Morahan (1996) 6q21 IDDM15 Delepine (1997)
Natural History of T1DM Popul islet-related Abs+ Follow- Risk References up Identical Twins 100%Tun RY, BMJ 1994 1st degree relatives (FH+) 70% ICARUS Group Study Polyendocrinopathy (FH-) 25% Bosi E, Diabetes 1991 Polyendocrinopathy (FH+) 70% Bosi E, Diabetes 1991 High risk newborns (FH+) 50% BABYDIAB (Germany) High risk newborns (gene+) 50% DIPP Project (Finland) Sardinian school children (gen) 24% SSI Study (Sardinia) 10 yrs 5 yrs 10 yrs 10 yrs 2 yrs 2 yrs 7 yrs
Natural history of T1DM tt Triggers ? Triggers ? Auto Abs + 75% FPIR 50% OGTT + Triggers ? Beta cell mass 25% GENES (susc) TYPE 1 DIABETES 0 Time
Screening for pre-T1DM and related AD •France • Sweden • Spain • Oxford • Holland • Estonia • SSI • USA • Finland • Germany Schoolchildren • DAISY (USA) • BABYDIAB (Germany, Australia) • SNI (Sardinia) • DIPP (Finland) • DIABFIN (Italy) Newborn
Cost of predicting T1DM • Conventional Therapy (CT) $1450 • Intensive Therapy (ICT) $ 2 x CT • CSII $ 3 x CT Cost of insulin therapies (per year) Cost of Screening (for each enrolled case) • DPT-1 $1751 • DIPP (follow up=10 yrs) • (newborns) $245 $733 Birth Birth Hahl et al. Diabetologia (1998) 41:79-85 100% 100% Genetic+Abs screening Abs screening 100% 13% Abs follow up Counselling Cost of DM (?AD) • $ 92 billions Abs follow up
T1DM&AD are theoretically preventable • Because there are environmental causes • Because we are beginning to understand the genetic and immune basis • Because they develops very slowly • Because we have good predictive tests • Because we can stop them in animals • Because we can run clinical trials
T1DM & AD are suitable diseases for preclinical screening and intervention • Serious consequences (in USA 50 deaths yearly from DKA) • Treatment following diagnosis expensive, demanding, limited effect on complications • Identifiable preclinical phase also for AD • Identifiable subjects “not at risk” also for AD • ...but as yet no preventive therapy of proved efficacy (no penicillin for prediabetes!)
Assigning risk • Primary prevention: must be based on family history or high risk HLA - and will miss a lot of cases! • Secondary prevention: immune-markers relatively stable after age 5; almost inevitable progression with multiple antibodies; excellent screening efficiency (islet imaging)
Setting up an intervention: in whom? • Primary: Neonates with family history or high risk HLA • Secondary: • Infants: HLA DR3/4 with antibodies • Children/young adults with multiple Abs (T1DM&AD) • Older adults with LADA
Setting up an intervention: with what? Should work: • In animal models • In newly diagnosed type 1 • In pilot trials (assessed how?) Must have: • An acceptable safety profile • Ease of administration
Setting up an intervention: conclusions • At present trials must be large, structured, costly and long term • Will depend on international collaboration • We need a disciplined consensus process for evaluating and prioritizing new therapies • Role of pharmaceutical industry? clinicians should have a say
T1DM prevention trials Primary Cow’s milk avoidance: TRIGR Gluten free diet: PREVFIN Secondary Nicotinamide: DENIS, ENDIT, New Zealand Insulin: DPT-1, EPLL SCIT; Schwabing, Brunetti 1999 Tertiary Cyclosporin: GETREM, French and Canadian studies Linomide : Franco-Swedish trial
Intervention trials: assumptions Trial N Yr Diabetes RRR % % ENDIT 530 5 40:26 35 DENIS 130 3 30:6 80 DPT (high) 340 4 84:55 35 DPT (inter) 490 4 24:12 50 Mahon and Dupre,1997
Cyclosporin before onset of T1DM • 6 relatives vs 9 historical controls • All controls developed diabetes in 12 months • 4/6 cyclosporin treated patients developed diabetes within 4 years (5, 24, 24 and 47 months) Carel et al., 1996
Intervention in early infancy? • Level of risk? • Safety of intervention? Long term data? • Acceptability/compliance? • Efficacy demonstrated in other AD? • Can the intervention be tested effectively in this category of patient?
Emergence of at least one auto-Ab by the age of 2 years (n=173) FOLLOW-UP, MONTHS 3 6 9 12 18 24 TOTAL CASEIN 0/83 0/75 1/72 3/71 1/67 1/62 3/84 HYDROLYSATE (3.6%) p=0.06 CM-BASED 0/87 1/84 6/79 7/78 6/77 7/76 10/89 FORMULA (11.2%) The Second TRIGR Pilot Study
EURODIAB Sardinia (1989-98)birth seasonality P<0.001 Jan-March Apr-June Jul-Sept Oct-Dec N=1928, 0-29yr
Future Directions? • Surrogate end-points • Safety and acceptability need to be balanced against efficacy • Early “one-off” therapy would be ideal • Explicit standards for performance of trials • Fewer, better quality studies based on international consensus • Lessons from other human autoimmune disease?