Download
1 / 39
430 likes | 918 Views
Gallbladder & Biliary Ducts. פואד משרקי מדריך קליני מח' כירורגית מרכז רפואי בני-ציון. Biliary System. Anatomy of Biliary Ducts. Anatomy of Gallbladder. Pear-shaped, hollow, saclike organ. 7.5 – 10 cm long.

E N D
Gallbladder&Biliary Ducts פואד משרקי מדריך קליני מח' כירורגית מרכז רפואי בני-ציון
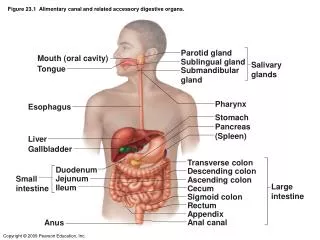
Anatomy of Gallbladder Pear-shaped, hollow, saclike organ. 7.5 – 10 cm long. Lies in a shallow depression on the inferior surface of the liver attached by loose connective tissue. Capacity 30 – 50ml of bile. Gallbladder wall smooth muscle. Connected to CBD by cystic duct.
What is a Gallbladder? ♦Organ in the body, responsible for: ◊concentrating & ◊storing ♦ Sits just under the liver in the upper Rt. Side of the abdomen “RUQ” BILE
Physiologic Overview A storage depot for bile: large portion of the water in bile is absorbed through the wall of gallbladder bile into the gallbladder become concentrated 10 time more than originally secreted by liver. Food Duodenum CCK-PZymin Gallbladder contracts & Sphincter of oddi relaxes Bile enter the intestine.
What is Bile? ♦ Digestive juice made by the liver. ♦ Responsible for helping the body to digest fats and fatty foods in our diet. ♦ NormallyGolden color ♦¼ - 1¼ Liters of bile each day.
What is Bile? ♦ Bile composed of: ► Water ► Electrolytes: Na, K, Ca, Cl, HCO3 ► Fatty acids ► Cholesterol ► Billirubin ► Bile salts Blood supply Cystic Artery (RHA)
What are the bile ducts? ♦Size of a small straw or pencil. ♦ Link the liver to the gallbladder and conduct the bile into for future use. ♦ By them, the bile passes to the digestive system.
Disorders of the G.B. Disorders bile drainage ☺Inflammation of the biliary system ☺Gallstones cholelithiasis, cholecystitis ☺Carcinoma 90% of patients with acute cholecystitis have G.S. % of people with G.S. have no pain
CHOLECYSTITIS Acute inflammation of G.B. causes:pain, tenderness, rigidity of RUQ +/- radiation to midsternal area or Rt. shoulders associated with nausea, vomitings and inflammation signs, empyema and pus.
CHOLECYSTITIS Calculous Cholecystitis 90% Acalculous Cholecystitis 10%
Calculous Cholecystitis Stone obstructs bile outflow stasis of bile empyema, pus, gangrene, perforation Escherichia coli (e.coli) 60% Klebsiella 22% Streptococcus 18%
Acalculous Cholecystitis ♦ sever trauma ♦ major surgical procedures ♦ burns ♦ torsion ♦ cystic duct obstruction ♦ multiple blood transfusion
The 4 Fs Female Forty Fatty Fertile Uncommon in children
Pathophysiology 2 major types of G.S. Pigment25% Cholesterol75% Pigment stones reasons: cirrhosis hemolysis biliary tract infections Cholesterol stones: normal constituent of bile
Risk factors for cholelithiasis ► obesity ► women – multiple pregnancies ► frequent changes in weight ► rapid weight loss ► treatment with high dose of estrogen ( (Ca of prostate) ► ileal resection or disease ► cystic fibrosis ► diabetes mellitus
Clinical manifestations ♦Silent ♦Mild gastrointestinal symptoms ♦ Vague pain RUQ ♦Epigastric distress after fatty foods ♦Fullness ♦Jaundice CBD obstruction
Pain & Biliary colic Obstruction of cystic duct by stone… G.B. becomes distended, inflamed, fever, palpable abd. Mass, nausea, vomitings, restlessly. G.B. contacts the abd. Wall / Rt. Costal cartilages deep inspiration pain. Requirs analgesics… MO is not recommended spasm of Oddi sphincter.
Obstruction JAUNDICE Total bill. > 1.2 Direct bill. > 50% Alkaline phosphatase AST, ALT, GGT levels rise moderately Feces: grayish, like putty, clay-colored. Urine: very dark color excretion of the bile pigments by kidneys.
Diagnostic findings X-Ray:only 15 – 20% of G.S. arecalcified sufficiently to be visible. US: diagnostic procedure of choice, rapid, accurate, can be used in patients with jaundice and liver dysfunction, no ionizing radiation. Most accurate (95%) patient in fast (distended G.B.) EUS: accurate 95% ERCP: direct visualization to CBD Endoscopic Retrograde Cholangiopancreatography
Nursing implication Before procedure: ♦ Explanation of the procedure. ♦ Patient should be in fast. ♦ Moderate sedation: opioid, benzo. ♦ Monitoring the patient. ♦ I.V. fluids. ♦ Administers medications. ♦ Observing sings of respiratory & CNS ddepression: hypotension, vomitings. ♦ Positioning the patient. ♦ Anticholinergics: glucagon
Nursing implication After procedure: ♦ Monitoring the patient’s condition. ♦ Observing vital sings. ♦ Monitoring side effects of medications: gag & cough reflexes. ♦ Monitoring sign of: perforation infection & sepsis pancreatitis bleeding (PTC) ♦ promptly report the physician if…
Laparoscopic Cholecystectomy Dramatically changed the approach to the management of cholecystitis. New standards for therapy of symptomatic G.S. 500,000 patients in the U.S.A CBD Obstructed ERCP Lap. cholecystectomy
Information should be givenabout the surgery ♦ Laparotomy maybe necessary ♦ General anesthesia ♦ Small punctures in the abdomen ♦ Co gas ♦ Cystic duct is dissected ♦ Cystic artery is dissected and clipped ♦ G.B. is separated from hepatic bed and d dissected ♦ Bile and stones are aspirated ♦ G.B. is removed
Advantages of laparoscopy ♦ No experience of paralytic ileus ♦ Less postoperative abdominal pain ♦ Discharging from hospital into 1 – 2 jjdays ♦ Full activity and employment within 1 week
Complications CBD injury bile leak bile peritonitis critical illness and/or death
Drainage T-TUBE: choledochostomy CHOLECYSTOSTOMY: poor risk for surgical procedure or for general anesthesia such as sepsis, CHF, pulmonary failure, acute MI.
Nursing process Assessment: ♦ admitting to the hospital ♦ preadmission testing (ECG, X-Ray, Blood chemistry, hematology and coagulation studies) ♦ stop smoking: ► enhance pulmonary recovery ►postoperatively ► avoid respiratory complication ♦ stop aspirin
Nursing process Instructions & Goals: ♦ Being in fast from 24mn ♦ Getting premedications: valium, pramin ♦ I.V. fluids & abx ♦ Relieving pain ♦ Adequate ventilation ♦ Absence of complications ♦ Self-care
Postoperative Nursing ♦ Recovery from anesthesia ♦ Fowler’s position ♦ Monitoring vital signs, pain & signs of blbleeding ♦ I.V. fluids ♦ Keep fasting ♦ Pass urine ♦ Water within hours ♦ Soft diet after bowel sounds/evening
Relieving pain As soon as possible (I.V.) Enable: turning, moving, deep breathing, coughing and preventing postoperative complications. Nurse administers analgesic agents as prescribed in order to relief pain and promote well-being. Using pillow/binder reducing pain
Improving respiratory status Nurse reminds patient to take deep breath and to cough. Using spirometry and improving respiratory functions. Early ambulation prevents pulmonary complications as well as others like thrombophlebitis.
Managing self-careHome & Community Nurse teaches and instructs patient aboutmedications (ABX) and their side effects. Symptoms should be reported: jaundice, dark urine and pale colored stools. Wound healing: wash puncture site daily, check puncture site, color, local fever, bad smell and oozing. Severe pain and signs of infection should be reported.
Managing self-careHome & Community ♦ Pulmonary exercises and cough. ♦ Gradual return to normal activities. ♦ Avoiding lifting heavy objects for 1 week. ♦ Sexual activity when desired. ♦ Normal diet. ♦ Pain relief: shoulders and abdomen. ♦ Make an appointment with surgeon for 7–10 days after discharge.
מושגים בנושא כיס מרה CHOLECYSTITIS ♦דלקת בכיס המרהCHOLECYSTITIS ♦אבנים בכיס המרהCHOLELITHIASIS ♦כריתת כיס המרהLAP/OPEN CHOLECYSTECTOMY ♦דלקת דרכי המרהCHOLANGITIS ♦דרכי מרה משותפותCBD: COMMON BILE DUCTS ♦דלקת של דרכי המרה המשותפותCHOLANGITIS ♦ אבנים ב- CBDCHOLEDOCHOLITHIASIS ♦ פתיחת ה- CBDCHOLEDOCHOTOMY ♦פתיחת ה-CBDוהסרת אבניםCHOLEDOCHOLITHOTOMY ♦השקת ה-CBDCHOLEDOCHODUODENOSTOMY ♦החדרת נקז לכיס המרהCHOLECYSTOSTOMY ♦כיס מרה נפוח ומלא הפרשותHYDROPS ♦כיס מרה מלא מוגלהEMPYEMA CHOLELITHIASIS LAP/OPEN CHOLECYSTECTOMY CHOLANGITIS CBD: COMMON BILE DUCTS CHOLANGITIS CHOLEDOCHOLITHIASIS CHOLEDOCHOTOMY CHOLEDOCHOLITHOTOMY CHOLEDOCHODUODENOSTOMY CHOLECYSTOSTOMY HYDROPS EMPYEMA
SEEU AT SURGERY SECTION