Download
1 / 24
240 likes | 261 Views
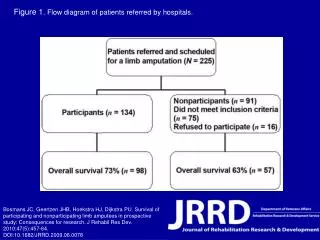
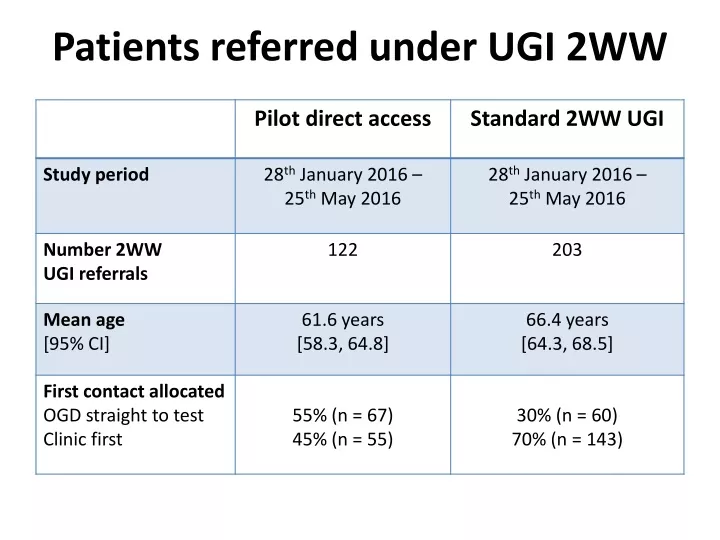
Study compares direct access and standard 2WW pathways for UGI patients at NUH, highlighting time to first contact, test requests, and cancer diagnoses. Findings support efficient exit strategies.

E N D
Time to first contact at NUH: OGD No difference between pilot direct access and standard 2WW p > 0.05
Time to first contact at NUH: clinic No difference between pilot direct access and standard 2WW p > 0.05
Time on UGI 2WW pathway Exit from UGI 2WW pathway may involve: • test(s) undertaken to diagnose patient’s symptoms • test(s) performed to exclude oesophago-gastric cancer
Time on UGI 2WW pathway No difference between pilot direct access and standard 2WW p > 0.05
Time on UGI 2WW pathway Quicker exit time from UGI 2WW pathway if only contact is straight-to-test OGD -> Caveat: test to exclude OG cancer
Time on UGI 2WW pathway Quicker exit from UGI 2WW pathway along standard UGI 2WW p < 0.05
Emergency presentation resulting in a diagnosis of cancer at NUH in 2014 Number of cancers diagnosed following emergency admission to NUH Postcode
Postcode distribution? Proportion %
Conclusions • Vetting at hospital stage is not rate limiting step in exit from pathway
Conclusions • Vetting at hospital stage is not rate limiting step in exit from pathway • Cancers identified by GP-requested DTT OGD were not oesophago-gastric but required further tests
Conclusions • Vetting at hospital stage is not rate limiting step in exit from pathway • Cancers identified by GP-requested DTT OGD were not oesophago-gastric but required further tests • UGI 2WW pathway more frequently diagnoses cancer outside of oesophago-gastric tract [which cannot be diagnosed by OGD alone]
Conclusions • Vetting at hospital stage is not rate limiting step in exit from pathway • Cancers identified by GP-requested DTT OGD were not oesophago-gastric but required further tests • UGI 2WW pathway more frequently diagnoses cancer outside of oesophago-gastric tract [which cannot be diagnosed by OGD alone] • There is a postcode variation in 2WW suspected cancer referrals and emergency cancer diagnoses but this is complex
Conclusions • Vetting at hospital stage is not rate limiting step in exit from pathway • Cancers identified by GP-requested DTT OGD were not oesophago-gastric but required further tests • UGI 2WW pathway more frequently diagnoses cancer outside of oesophago-gastric tract [which cannot be diagnosed by OGD alone] • There is a postcode variation in 2WW suspected cancer referrals and emergency cancer diagnoses but this is complex
Nina R Lewisnina.lewis@nuh.nhs.uk0115 9691169 Extension 56335Fax: 0115 8405821