Download
1 / 48
480 likes | 639 Views
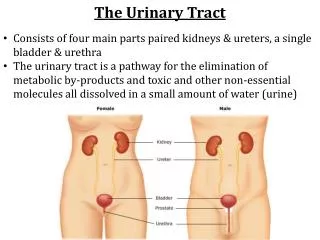
Urinary tract infections in men: the classical urovirulent E. coli?. Peter Ulleryd Regional Medical Officer Communicable Disease Control Västra Götaland, Sweden peter.ulleryd@medfak.gu.se. Professor????. No!. Co-workers.

E N D
Urinary tract infections in men:the classical urovirulent E. coli? Peter Ulleryd Regional Medical Officer Communicable Disease Control Västra Götaland, Sweden peter.ulleryd@medfak.gu.se Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Professor???? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
No! Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Co-workers Torsten Sandberg Infectious Diseases, Sahlgrenska University Hospital Jonas Hugosson, Gunnar Aus, Svante Bergdahl and Björn Zackrisson Urology, Sahlgrenska University Hospital, Göteborg Knut Lincoln Clinical Bacteriology, Sahlgrenska University Hospital Flemming Scheutz The international E. coli and Klebsiella centre (WHO), Copenhagen James R. Johnson VA Medical Center, Minneapolis Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Cross-talk • Not only important for bacteria • Also for people working with: • E. coli • UTI • Antibiotic resistance • etc Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Menu • Primitive creatures • UTI - classification • Febrile UTI in men - clinic • Virulence factors Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Clinicians-primitive creatures! • Internal medicine vs Surgeons • Is this of any good for my patients? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Giving a diagnosis • X no. of symptoms/signs=diagnosis • The most usual is the most abundant! • Ex. Fever + bacteriuria Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Bacterial virulence factors:are they important to know for the treating physician? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
No! Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Just UTI - define!! • Women Men Children • Asymptomatic Symptomatic • Febrile UTI Lower UTI • Sporadic Recurrent • Complicating factors Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Virulence Host factors Infection No infection Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
UTI in men Traditionally - anatomic abnormalities in the newborn - prostatic obstruction in the elderly • Most UTI in men are complicated • Less E. coli than in women • Often Pseudomonas, Serratia, enterococci……… Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Male UTI • Lower UTI = ”Cystitis” • Febrile UTI = ”Upper” UTI = ”Pyelo.” • Prostatitis – Acute, Kron bact., Kron abact., Prostatodynia • Urethritis Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Febrile UTI in men-the Gothenburg prospective study Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Inclusion criteria • Temperature 38.0°C • Clinical signs/symptoms of UTI • Positive urine culture • 104 cfu/mL MSU Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Investigations • Transrectal ultrasound (TRUS) • Residual urine • Uroflowmetry • Urography • Cystoscopy • Prostate-specific antigen (PSA) At entry and after3 months During follow-up At entry and follow-up Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Characteristics of men with febrile UTI (n=86) Median age 63 years (18 – 86) Previous history of UTI 38 (44%) Flank pain and/or costovertebral angle 31 (36%) tenderness Median temperature 39.5°C (38.0 – 41.4) Median C-reactive protein 130 mg/L (9 – 420) Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Bacteriological findings in 86 patients with febrile UTI Urinary isolates Blood isolates Escherichia coli1 67 (78 %) 10 Klebsiella pneumoniae 7 Enterobacter aerogenes 1 1 Enterobacter agglomerans 1 1 Proteus mirabilis 1 1 Enterococci 4 Staphylococcus epidermidis 3 1 Group B streptococci 2 1 In one case together with Serratia marcescens Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
? Is the prostate frequently involved in men with febrile urinary tract infection? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Fig 2. Median serum PSA after an episode of febrile UTI 15 14.0 10 PSA (µg/L) 5 3.6 2.9 2.0 1.5 0 0 1 3 6 12 n=70 n=69 n=55 n=50 n=41 months Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Serum PSA after an episode of febrile UTI Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Prostate volume in 55 men with febrile UTI (range) • At entry • After 3 months 49 mL 35 mL (14 - 104 mL) (15 - 91 mL) Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Changes in serum PSA and prostate volumebetween the acute stage of infection and 3 months later in 49 men with febrile UTI Reduction in prostate volume >10% 10% Reduction in serum PSA >25% 40 4 25% 2 3 BJU Int 1999;84:470-4. Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
? Is the prostate frequently involved in men with febrile urinary tract infection? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Yes! Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Febrile UTI in men One infection – different manifestations Acute pyelonephritis Febrile UTI Acute prostatitis Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
? Is it always necessary to examine the upper and lower urinary tract after a febrile UTI? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Lower urinary tract abnormalities in 83 men with febrile UTI Abnormality No. (%) of findingsa Infravesical obstruction from BPH requiring TURP 10 Urethral stricture 5 Bladder diverticulum 5 Bladder stones 3 Bladder cancer 1 Phimosis 1 Post-void residual urine >50 mLb 13(22) Peak urine flow rate <10 mL/sb 8(15) a46 abnormal findings in 35 patients. bBased on the best performance during the acute stage or at follow-up. Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
? Is it always necessary to examine the upper and lower urinary tract after a febrile UTI? Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
No! Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Urological evaluation of male febrile UTI • Conclusion • Routine imaging of the upper urinary tract seem dispensable. • To reveal abnormalities of clinical importance, evaluation should primarily be focused on the lower urinary tract. • BJU Int 2001;88:15-20 Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Proposed urological evaluation of male febrile UTI • At 1 (+3 and 6) months: • Clinical control including urinary and obstructive symptoms • Dipstick for hematuria • Urine culture • Repetition of eventual abnormal laboratory tests • Post-void residual • Peak flow rate • DRE Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Treatment • Ab concentration in the prostate • High pH, calcifications, reflux • Quinolones, (trimethoprim), ((doxycycline)) to obtain ab in prostatic secretion Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Virulence characteristics of E. coli in febrile UTI MenWomen n=74Uncomplicated Complicated FU Hemolysin 74% 51% 41% P-fimbriae 51% 80% 65% Aerobactin 46% 73% Suggesting differences in host-parasite relationships in the male and female urinary tract. TS JJ CID 1994;18:579-84 Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Earlier studies of haemolysin in male UTI • Barnes RC,Daifuku R, Roddy RE, Stamm WE. Lancet, 1986. • 10/11 isolates • Spach DH, Stapleton AE, Stamm WE. JAMA1992. • 10/14 isolates Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Later studies of haemolysin in male UTI • Andreu et al 22/30 73% • Terai et al 72/107 69% • Ruiz et al 30/37 81% • CNF1 was also very commonly found • concomitantly with the haemolysin gene Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
FUTI urine (n=70) Uninfected, rectal (n=70) Prevalence of virulence factorsJR Johnson et al 2005 FUTI isolates exibited a significantly higher prevalence of virulence-associated phylogenetic groups, serotypes, and extraintestinal virulence genes. Including haemolysin and CNF-1 Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Comparison concurrent U+R isolatesJR Johnson et al 2005, n=65 • 3 last rectal isolates+morph distinct • Only the urine isolate in 25 % • Urine clone + additional clone in 22% • Only nonurine clones in 54% Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Figure 1. Distribution of virulence factor scores among concurrent urine (n = 65) and rectal (n = 67) Escherichia coli isolates from 65 men with febrile urinary tract infection. Only rectal isolates that differed clonally from the host's urine isolate are included in the rectal group. Fractional scores were rounded down to the next lowest integer value. Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Cytotoxic necrotizing factor type 1 (CNF1) • Contribute to prostatic inflammation by E. coli in a rat model. • Rippere-Lampere KE, Inf Imm, 2001. • However, another murine model, but female, demonstrated no evidence of CNF1- associated inflammation of the urinary tract. • Johnson DE, FEMS Imm, 2000. Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Febrile UTI in men One infection – different manifestations Acute pyelonephritis Febrile UTI Acute prostatitis Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Conclusions - general • Studies of very well characterized patients and bugs with specified infections (prospective) • Multidisciplinary in-/output of importance (cross–talk) Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Conclusions Male FUTI • E. coli of course. • Pathogenesis - Deep, Dip, Dep. • Do not take PSA. • If investigation - aim low. • Treatment for the prostate also. • Common sense allowed. Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden
Thank you! Peter Ulleryd, Sahlgrenska University Hospital, Göteborg, Sweden