Download
1 / 9
90 likes | 325 Views
Randomized Therapeutic Vaccine Trial of Canarypox-HIV (CP-HIV) + Dendritic Cells vs. CP-HIV Alone in HIV-infected Patients on Antiretroviral Therapy: ACTG A5130. ALVAC-HIV (vCP1452): CP vector that contains HIV env and gag genes and CTL epitopes from nef and pol .

E N D
Randomized Therapeutic Vaccine Trial of Canarypox-HIV (CP-HIV) + Dendritic Cells vs. CP-HIV Alone in HIV-infected Patients on Antiretroviral Therapy: ACTG A5130 • ALVAC-HIV (vCP1452): CP vector that contains HIV env and gag genes and CTL epitopes from nef and pol. • HIV+ subjects vaccinated with CP-HIV alone have small and transient increases in HIV-specific immunity. However, vaccination with CP-HIV in patients treated with ART during acute or chronic HIV infection does not lead to virologic control during treatment interruptionJacobsonJID 194:623; Kinloch-de Loes JID 192:607; Autran AIDS 22:1313 • Dendritic cells infected with CP-HIV elicit HIV-specific CD4 & CD8 immune responses in vitro Engelmayer. J Virol. 75:2142 • Hypothesis: Immunization of HIV+ patients on ART with DCs plus CP-HIV will be more immunogenic and lead to better control of viremia during a treatment interruption than vaccination with CP-HIV alone
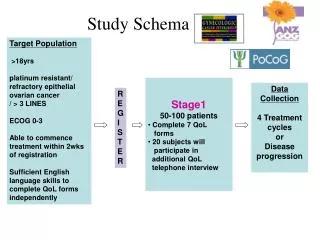
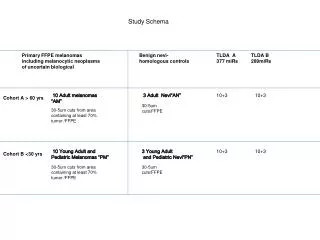
Study Schema 29 HIV+ Subjects On ART VL<50 CD4 > 400 Arm A DC+CP HIV N=14 12-week ATI. VL setpoint at end of ATI Arm B CP HIV N=15 1:1 Wk 3 Wk 7 Wk 15 = vaccination with DCs + CP-HIV or CP-HIV alone. At wks 3 and 7, subjects also received keyhole limpet hemocyanin (KLH). KLH was a control to determine whether priming of new immune responses occurred. Primary Endpoints: 1) VL setpoint at the end of a 12-week ATI; 2) Safety: ≥ grade 3 adverse event that is at least possibly related to study treatment.
Inject CP-HIV-infected DCs at wk 3, 7 & 15 (1.5 to 6 million DCs, SQ) HIV+ pt on antiretroviral therapy Infect with CP-HIV (ALVAC vCP1452) Mature DCs using cocktail of IL-1b, IL-6, TNF-a, PGE2 Isolate PBMC from leukapheresis product (1-3 billion PBMC) Expand monocyte-derived DCs using IL-4 and-GM CSF (7 days in a cell processing lab at MGH) Based on slide from Nina Bhardwaj, M.D., Ph.D.
Effect of Vaccination on LPA • Subjects who received KLH-pulsed DCs had a significantly greater increase in KLH LPA response prior to ATI than subjects who received KLH alone • Median SI fold change 5.7 in arm A vs. 1.8 in arm B, p=0.007 • No change in LPA response to tetanus, candida or 5 pools of HIV peptides A: KLH-pulsed DCs.B: KLH alone
Fold-increase in ELISPOT Responses During Vaccination Arm A (n=12) DC+ CP-HIV Arm B (n=12) CP-HIV alone • 5/12 (42%) subjects in arm A and 5/12 (42%) subjects in arm B had a >3-fold increase in summed ELISPOT response over baseline at 1 or more time points after vaccination and before ATI Responder: 3-fold increase in ELISPOT response that is also >30 SFC/million PBMC
Viral Load during ATI: Summary • No difference in VL setpoint between subjects in Arm A and B (medians 4.1 and 4.5 log10 c/mL) • 4/13 (31%) in DC+CP-HIV arm had VL setpoint <5,000 compared with 0/13 (0%) in CP-HIV alone arm (p=0.096) • Of the 4 subjects who achieved VL setpoint <5,000 at end of ATI, 2 had increase in VL to >5,000 on follow-up (7 wks later) Arm B (n=15) CP-HIV alone Arm A (n=14) DC+CP-HIV VL=5000 Setpoint VL <5000 c/mL
ELISPOT response and VL Setpoint during ATI • Summed ELISPOT level after vaccination negatively but weakly correlated with VL setpoint (not sig.) • Greater fold-increases in gag, nef or summed ELISPOT response after vaccination are associated with lower VL setpoint (all p-values <0.05)
Conclusions • CP-HIV & DC+CP-HIV therapeutic vaccines are safe and immunogenic in HIV-infected patients • DCs effective as an adjuvant to prime responses to KLH, but did not clearly enhance HIV-specific ELISPOT responses • Suggestion that subjects vaccinated with CP-HIV+DC had a higher rate of VL setpoint <5,000 c/mL during ATI than subjects immunized with CP-HIV alone; however, control was transient • Subjects who had higher fold-increases in HIV-specific ELISPOT responses after vaccination had lower VL setpoints • Further studies of the correlates of antiviral immunity and methods to more effectively boost antiviral immunity are warranted
Acknowledgments ACTG 5130 team • Jeff Jacobson, protocol chair; Rajesh Gandhi and Nina Bhardwaj, vice-chairs • David O’Neill, Ellen Chan, Ron Bosch • Pat Bucy, Mary Marovich, Lynn Baglyos, Reena Masih, Barbara Schock, Lynette Purdue and the 5130 team Massachusetts General Hospital • Teri Flynn, Amy Sbrolla, Janet Shopis, Kathy Habeeb, Nicole Burgett, Gil Roy, Daniel Kavanagh, Doug Kwon, Bruce Walker NYU Cancer Institute Vaccine Center • Crystal M. Cruz, Angelica Angiulli and Francesca Angiulli Burroughs Wellcome, Elizabeth Glaser, Doris Duke Beth Israel, NY • Ann Marshak, Gwen Constantini, Sondra Middleton, Donald Garmon, Scott Barnett, Donna Mildvan Study subjects at MGH and Beth Israel, NY