Download
1 / 22
1.87k likes | 7.36k Views
Pyloric Stenosis. Jie Chen,M.D, phD Children Hospital,ZJU. Gastric Outlet Obstruction. Hallmark is non-bilious vomiting Other signs include abdominal distention and bleeding from secondary inflammation Most common cause of non-bilious vomiting is infantile hypertrophic pyloric stenosis.

E N D
Pyloric Stenosis Jie Chen,M.D, phD Children Hospital,ZJU
Gastric Outlet Obstruction • Hallmark is non-bilious vomiting • Other signs include abdominal distention and bleeding from secondary inflammation • Most common cause of non-bilious vomiting is infantile hypertrophic pyloric stenosis
Pyloric Stenosis • First described by Hirschsprung in 1888 • Ramstedt described an operative procedure to alleviate the condition in 1907 – the procedure used to this day to treat pyloric stenosis
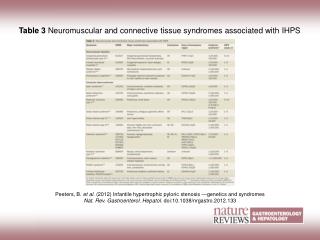
Pyloric Stenosis • 3/1000 live births – frequency may be increasing • Most common in whites of Northern European ancestry, less common in African Americans and rare in Asians • Four times more common in males – especially firstborn • Increased in infants with type B or O blood groups • Associated with other congenital defects incl TEF
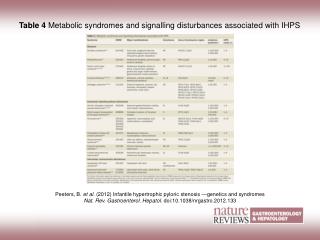
Etiology • Cause is unknown, but abnormal muscle innervation, breast feeding and maternal stress in the 3rd trimester have been implicated • Elevated serum PG’s, reduced levels of pyloric nitric oxide synthase and infant hypergastrinemia have been found
Clinical Manifestations • Non-bilious vomiting is the initial symptom • May or may not be projectile initially • Usually progressive, occurs immediately after a feeding • Vomiting usually starts after 3 wks of age, but may develop as early as 1st week and as late as the 5th month
Clinical Manifestations • After vomiting, infant is hungry and wants to feed again • Progressive loss of fluid, hydrogen ion and chloride leads to a hypochloremic metabolic alkalosis. • Serum K levels are maintained • Greater awareness has led to earlier diagnosis
Clinical Manifestations • Jaundice occurs in 5% of infants with pyloric stenosis – associated with a decreased level of glucuronyl transferase
Clinical Manifestations • Diagnosis traditionally made by palpation of mass • Firm, movable, approx 2 cm in length, olive shaped and best palpated from the left • Mass located above and to the right of the umbilicus in the midepigastrum beneath the liver edge • Peristaltic wave may be present prior to emesis
Diagnosis • Straightforward if olive is present • Difficult to distinguish from GERD esp in early stages • UGI or US can be used – but US has become the standard at most centers • Ultrasound – Sensitivity of 90% • Criteria for diagnosis – pyloric muscle thickness greater than 4 mm and an overall pyloric muscle length greater than 14mm
Diagnosis • US pitfalls – pylorospasm may mimic those of PS, potential false-pos and false-negative readings • UGI – classic signs are elongated pyloric canal, the “double tract” sign (parallel streaks of barium in the narrowed channel, and the “shoulder sign”(bulge of pyloric muscle into the antrum). • Main pitfall of UGI is radiation exposure
(1)幽门管细长,呈“线样征” 十二指肠球底见“蕈伞征” (2)幽门管内可见“双轨征” (3)胃窦部幽门前区“鸟嘴征
Differential • Infants who are reactive to external stimulation, those fed by inexperienced caretakers, or those for whom adequate maternal-infant bonding has not been established may vomit frequently in the early weeks of life. • GERD with or without a hiatal hernia may be confused with PS esp in the early stages
Differential • Inborn errors of metabolism may produce recurrent emesis with alkalosis or acidosis and lethargy, coma or seizures. • Salt-losing CAH presents with prominent vomiting shortly after birth. Females will be virilized, but the genitals appear normal in males. Acidosis and hyperkalemia usually present.
Differential • Vomiting with diarrhea suggests gastroenteritis. • Always have to think of increased ICP, subdural hematoma • Systemic infections can also cause persistent vomiting.
Treatment • Preoperative treatment is directed toward correcting the fluid/acid-base and electrolyte imbalances. • Correction of the alkalosis is essential to prevent postoperative apnea • Surgery is the treatment of choice – Ramstedt pyloromyotomy
Treatment • Ramstedt pyloromyotomy – performed through a short transverse incision or laparoscopically • Underlying pyloric mass is split without cutting the mucosa and the incision is closed • Post-op vomiting occurs in ½ the patients and thought to be due to edema of the pylorus • Feedings can usually be initiated within 12-24 hours
Treatment • Persistent vomiting suggests an incomplete pyloromyotomy, gastritis, GERD. • Surgical treatment is curative with a low mortality rate