Download
1 / 25
330 likes | 980 Views
Dr . S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics Ph d (physiology) Mahatma Gandhi medical college and research institute , puducherry – India . Pyloric stenosis. Incidence .

E N D
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics Ph d (physiology) Mahatma Gandhi medical college and research institute , puducherry – India Pyloric stenosis
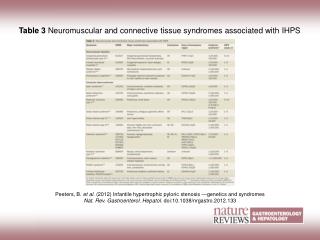
Incidence • Pyloric stenosis is one of the most common gastrointestinal abnormalities presenting in the first 6 months of life • 4 times more commonly in males • 1.4 to 8.8:1000 live births
Cause ?? • maternal postnatal exposure to macrolides?? • associated with cleft palate and esophageal reflux.
Clinical features • projectile vomiting, visible peristalsis, and a hypochloremic, hypokalemic, metabolic alkalosis. • Average 3 weeks of age • Non bilious vomiting
H+Cl-K+ obstn
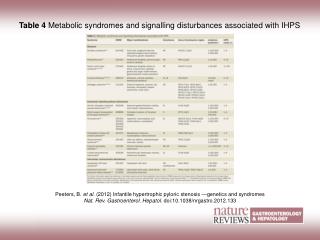
Clinical features • gross thickening of the circular muscles of the pylorus • Acidic secretions + chloride + potassium • Loss • -- hence • hypochloremic, hypokalemic, metabolic alkalosis. • Compensate – bicarb loss in urine
Clinical features • With persistent vomiting and intravascular volume depletion stimulates rennin angio- aldosterone to conserve Na for H+ to produce aciduria and worsens alkalosis • A palpable olive mass • Actively hungry child – initially
Think !! • Pyloric stenosis is an emergency case to intervene • But not an emergency to operate
Start?? • The initial therapeutic approach is aimed at repletion of intravascular volume and correction of electrolyte and acid-base abnormalities • Na+ K+Cl- HCO3 – • Gastric 70 5-15 120 0
Deficit correction • Initial • 0.9% NS (RL – lactate to bicarb ??) • 10 ml /kg over 4-6 hours • May need upto 40 ml/kg • Maintanence • 5% dextrose with 1/4th NS - 6 ml/kg /hour • If Renal function is ok , • 5% Dx with 1/4th NS with 4o mmol K+ - 6 ml/kg /hour
When to take up?? • Check for signs of good hydration (alertness, skin turgor, fontanelles, vital signs). Aim for • pH around 7.4, • Na > 132 mmol/L, • Cl > 90 mmol/L, • K > 3.2 mmol/L and • HCO3 around 25 mmol/L. • 24 -48 hours
Alkalosis can do • Shift of ODC to left • 70 % FHB, P50 22 approx • Decreased ionized calcium and propensity for seizures
Preop • Nasogastric tube and aspiration in the supine, lateral, and prone positions • Sometimes Barium • CBC,BUN, electrolytes, ABG, ECG(hypokalemia), • blood grouping • Urine output • Atropine 0.01 mg/kg
Induction • Newborn rapidly desaturates following only 15–20 seconds of apnea • Inh. Induction • 50 % O2 and 50 % N2O with 1.5 % halo • Or sevoflurane • Intubate without muscle relaxant if possible.
Some follow rapid sequence • Atropine 0.15 mg • Preoxygenation • 20 ml/kg bolus RL • Thio 4 mg/ kg Fent / suxa 1.5 mg/kg Cricoid pressure and intubation Less traumatic , less brady )
Airway differences • Infants younger than 6 months are obligate nose breathers • Lymphoid tissue prevents unobstructed nasopharyngeal airway placement • The tongue is relatively large • larynx is anterior and more cephalad in the • Newborn ( c2 C3) • The infant’s epiglottis is omega shaped, floppy,( may need Miller blade ) • Narrowest is cricoid ( uncuffed)
Tubes • Usually 3 or 3.5 mm Upto 10 cm Tube size 4 + age/4 Length = 14 + age /2
“1-2-3...7-8-9” rule • In neonates bronchial intubation extremely likely • To minimize this risk, use the • “1-2-3...7-8-9” rule to assist in correct • endotracheal tube positioning. • 1 kg ---- 7 cm • 2 kg ----- 8 cm • 3 kg ------ 9 cm
Ryle tube A small volume of air is injected down the nasogastric tube surgeon manipulates the air bubble into the duodenum occludes the bowel lumen both proximal and distal to the incision. Mucosal perforation is indicated if there is air leakage. the operation usual less than 30 minutes
Maintenance • N2o, O2 with halo/sevo , atracurium - JRMATP • Remifentanil is a unique potent opioid in neonates. • Maintain IVF (1/5thDx NS 4 ml/kg/hour), • urine output, • temperature • Extubate awake and smooth • Post op IVF till patient takes good oral intake
Post op • Increased risk for respiratory depression and hypoventilation in the recovery room because of persistent metabolic or cerebrospinal fluid alkalosis.
Postop pain care • Postop analgesia by local infiltration - bupivacaine(maximum dose, 1 mL/kg of 0.25% bupivacaine) acetaminophen (40-mg/kg initial dose followed by 20 mg/kg every 6 hours rectally or 10 mg/kg by mouth -- 4 to 6 hours 24-hour • ( total dose of ∼100 mg/kg).
The gist - intervene?? • (1) a full stomach, occasionally filled with contrast material • (2) metabolic alkalosis with hypochloremia and hypokalemia • (3) severe dehydration. • Rehydrate NS, 1/5th NS with Dx with K+, • NG aspiration • inh, ind. Controlled ventilation • Recover awake,postop pain
THANK YOU