Download
1 / 21
210 likes | 449 Views
Current Role of Partial Cystectomy: Are we scarifying patient ’ s survival. Dr Eric Li Department of Surgery Pamela Youde Nethersole hospital. Bladder tumor. TCC bladder (90%) SCC bladder (7-9%) Adenocarcinoma (1-2%) Sacroma Small cell carcinoma Urachal carcinoma. Gading of TCC .

E N D
Current Role of Partial Cystectomy: Are we scarifying patient’s survival Dr Eric Li Department of Surgery Pamela Youde Nethersole hospital
Bladder tumor • TCC bladder (90%) • SCC bladder (7-9%) • Adenocarcinoma (1-2%) • Sacroma • Small cell carcinoma • Urachal carcinoma
Gading of TCC • Degree of anaplasia of the tumor cells • correlation exists between tumor grade and stage Jewett and Strong, 1946 • correlation between tumor grade and prognosis • low-grade tumors and high-grade tumors have fundamentally different originsKnowles et al, 1994 ; Spruck et al, 1994 ; Reznikoff et al, 1996 ; Cote and Chatterjee, 1999
Staging of TCC (1997 AJCC-UICC, TNM Staging ) • Ta: Papillary, epithelium confined • Tis: Flat carcinoma in situ • T1: Lamina propria invasion • T2a: Superficial muscularis propria invasion • T2b: Deep muscularis propria invasion • T3a: Microscopic extension into perivesical fat • T3b: Macroscopic extension into perivesical fat • T4a: Cancer invading pelvic viscera (e.g., prostatic stroma, vaginal wall, rectum, uterus) • T4b: Extension to pelvic sidewalls, abdominal walls, or bony
Staging of TCC • N0: No histologic pelvic node metastases • N1: Single positive node ≤2 cm in diameter, below common iliacs • N2: Single positive node 2-5 cm in greatest diameter or multiple positive nodes • N3: Positive nodes >5 cm in diameter • Nx: Nodal status unknown • M0: No distant metastases • M1: Distant metastases documented • Mx: Distant metastases status uncertain
PATTERNS OF DISSEMINATION • Direct Extension • Lymphatic spread • Vascular spread • Implantation
Biology of TCC • Multicentric Origin • Clonal • Field change • almost all patients who develop metastases develop muscle-invasive recurrences before or at the time metastases are recognizedJewett and Strong, 1946 ; Freeman et al, 1995a
Treatment decision • Superficial versus Infiltrating Tumor?
Non-muscle invasive TCC • Transurethral Resection of Bladder Tumor (TURBT) • Intravesical Therapy • BCG • Mitomycin C
Muscle Invasive TCC • Radical Cystectomy • En bloc cystectomy • Bilateral pelvic iliac lymph node dissection • Urinary diversion
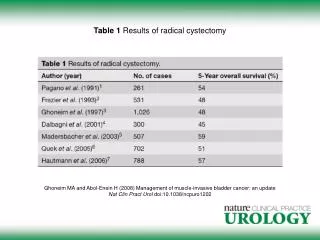
Radical cystectomy • 69% recurrence-free survival at 5 years • 60% overall survival at 5 years • Survival significantly related to pathologic stage and lymph node status • 9% overall local pelvic recurrence Donald G. Skinner 2007
Other treatment modality • Radiation Therapy • Transurethral Resection ( TUR) • Combined modality therapy
Partial cystectomy • Lower surgical risk • Preservation of bladder function • Preservation of sexual function • ??Scarifying survival
Results of Partial cystectomy • 58 patients undergone Partial cystectomy for primary bladder tumor from 1995 to 2001 in MSK Cancer Centre analyzed • Overall 5-year survival 69% • Concomitant CIS and multifocality at high risk of recurrence J M Holzbeierlein et al 2004
Results of Partial Cystectomy • 37 Patients with muscle invasive urothelial carcinoma underwent partial cystectomy with curative intent in M.D. Anderson Cancer Center • 5-year overall survival rate 67% • Higher pathological stage was associated with shorter recurrence-free survival • Lifelong followup with cystoscopy is recommended W Kassouf et al 2006
highly selective patient • Solitary mass • No concomitant CIS • Adequate surgical margin • Functional bladder Brannan et al, 1978
Conclusion • Radical cystectomy remain standard therapy of muscle-invasive urothelial bladder cancer • Survival rate of highly selected patient who undergo partial cystectomy is comparable to those with radical cystectomy • Lifelong survelliance is required for patient underwent partial cystectomy