Download
1 / 19
• 190 likes • 434 Views
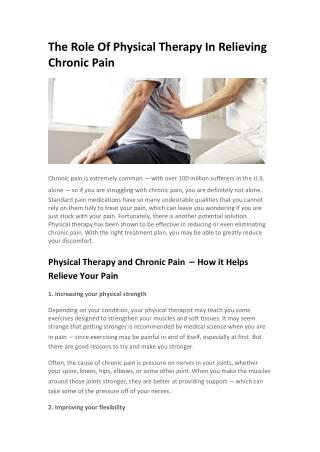
Hypolipidemic agents in chronic therapy. A compliance study in the ASSET cohort. The issue. In the 2000-2004 five years period, the Italian SSN invested cumulatively over €3.3. billion to fund the prescribing of statins in primary care [1].

E N D
Hypolipidemic agents in chronic therapy. A compliance study in the ASSET cohort
The issue • In the 2000-2004 five years period, the Italian SSN invested cumulatively over €3.3. billion to fund the prescribing of statins in primary care [1]. • Based on the Framingham coronary prediction algorithm, the expected return on this considerable investment would be a significant reduction of the Italian population’s risk for Coronary Heart Disease (CHD)
Statins yield a lower than expected return [2] • The observed 2000-2005 trend of hospital admissions for AMI seems to confirm the concerns raised by the Majeed et al. about the prescribing of lipid regulating drugs in England. [3]
Caveats • While the Framingham algorithm is based on a 10 years risk assessment, the observation period of analysis was significantly shorter • While we adjusted for ageing population, the impact of other important cardiovascular risk factors, such as cigarette smoking habit, blood pressure and diabetes, was ignored • We used hospital admissions for acute myocardial infarction as a proxy of Coronary Heart Disease: angina pectoris and coronary disease admissions were ignored to avoid double counting.
Statins’ DDD growth offsets the impact of generic substitution [1] € 1 billion/ year
Compliance: previous research • 2002: in the ASSR Umbria the medianpersistence on statins treatment was 5.3 months [4] • 2005: in the Pavia ASL the meanexposure to statins was > 180 days/year for 70% of treated patients [5] • 2005: in the ASSR Emilia-Romagna statins’ coverage was 46% [6]
A closer look at compliance:the ASSET [7] statins compliance study
The ASSET cohort • Integration of 2 databases: • Pharmaceutical individual costs • Personal data • Sample: 3,175,691 Italian residents • Timeframe: 24 months (January 04/ December 05) • Data collected: • Age • Sex • Drugs prescribed (ATC 5° level) • Cost paid by the Italian National Health Service (SSN) • Data privacy: all personal information were replaced by an univocal numerical code
Study objective [8] Evaluate the % of persistent and compliant subjects twelve month after initiating statins’ treatment Persistence: rate of subjects without an interval between 2 consecutive Rx < DDDs prescribed + 30 days Compliance: rate of persistent subjects with total number of DDDs prescribed/365 > 80% KEY ASSUMPTION: 1 pill = 1 DDD
Method • Jan 04-Mar 04 Wash out period equivalent to 2 Rxs x 24 days + 30 days (no carry over) • Apr 04-Sep 04 Enrolment period. Subject eligibility criterion: 0 statin Rx in Jan-Mar & at least 1 in the enrolment period • Oct 04-Sep 05 Observation period
Results • Out of the 33,139 patients enrolled, only 7% were persistent and 6% compliant (84% of persistent) • The % of persistent patients rapidly increases by relaxing the time interval between consecutive RXs, while the % of compliant patients is much less elastic to time interval of RXs. • 13,400 patients (40.4% of total) did not receive any Rx in the observation period
Skewed Rx distribution • >40% of enrolled patients with 0 Rx in the 12 month observation period • >50% with 1 • 80% with 5 or less
Multiple risk factors do not seem to significantly improve compliance to statins Diabetes and high blood pressure identified by the use of concomitant medications (ATC A10 and C)
Compliance cost • Compliant patients show a mean statins’ cost significantly higher compared to the total mean: • If every patient were compliant, the SSN burden would potentially quadruple • It is conceivable that 80% of the current statins’ prescribing cost has a limited impact in reducing the cardiovascular risk of the Italian population
Conclusions • The ASSET cohort shows a mean compliance rate to statins’ treatment significantly lower than expected on the basis of previous pharmaco-epidemiological studies • This is possibly due to the definition of compliance rate adopted • The compliance rate observed in the ASSET cohort • provides a possible explanation to the disappointing yield of the SSN investment on statins • raises the issue of moral hazard in the prevention of cardiovascular risk • points out the policy implications for a sustainable prevention of cardiovascular risk: • rational prescribing • reimbursement subject to compliance
References [1] Agenzia Italiana del Farmaco AIFA. L’uso dei farmaci in Italia. OSMED reports 2000-2004. Available online at: http://www.agenziafarmaco.it/aifa/servlet/section.ktml?target=&area_tematica=ATTIVITA_EDITORIALE§ion_code=AIFA_PUB_RAP_OSMED&cache_session=true [2] Favato G and Print C (2008). 2002 mortality rate for coronary heart disease in Italy: a statistical outlier or a sentinel event? Heart, Feb 27. Available online at: http://heart.bmj.com/cgi/eletters/94/2/178#8103 [3] Majeed A, Aylin P, Williams S, Bottle A, Jarman B (2004). Prescribing of lipid regulating drugs and admissions for myocardial infarction in England. BMJ, 2004 329:645, doi: 10.1136/bmj.329.7467.645 [4] Lucioni C, Mazzi S, Cerra C et al (2006), Uno studio di Drug Utilisation delle statine nella recente prassi terapeutica italiana. PharmacoEconomics-IRA. 8(1): 3-17 [5] Abraha I, Montedori A, et al (2003), Statin compliance in the Umbrian population. European Journal of Clinical Pharmacology. Vol. 59 Numbers 8-9. [6] Poluzzi E, Strahinja P, Lanzoni M, Vargiu A, Silvani M C, Motola D, Gaddi A, Vaccheri A, Montanaro N (2007). Adherence to statin therapy and patients’ cardiovascular risk: a pharmacoepidemiological study in Italy. Eur J Clin Pharmacol [7] Favato G, Mariani P, Mills RW, Capone A, Pelagatti M, et al. (2007) ASSET (Age/Sex Standardised Estimates of Treatment): A Research Model to Improve the Governance of Prescribing Funds in Italy. PLoS ONE 2(7): e592. doi:10.1371/journal.pone.0000592 [8] Larsen et al.(2002), High persistence of statin use in a Danish population: compliance study 1993-1998, British Journal of clinical Pharmacology, Vol 53, 4: 375-378