Download
1 / 55
550 likes | 564 Views
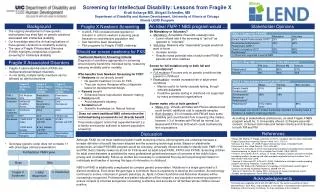
Explore the intersection of population, fragility, and health in conflict zones through real-world examples from Rwanda and Sierra Leone, highlighting the impact of health services on state stability and community resilience.

E N D
Health Service Delivery in Fragile States:Lessons from the Field Emmanuel d’Harcourt International Rescue Committee Woodrow Wilson Center for Scholars September 12, 2006
Outline • Population and fragility • Fragility and health • Health and fragility • Missions, health, and fragility
Outline • Population and fragility • Fragility and health • Health and fragility • Missions, health, and fragility
… The [demographic] "wolf" is present and very busy indeed—in Rwanda. … When its population had reached 7.6 million in 1994, observers there were expecting disaster any day in the form of random violence or famine … Rwanda is demographically trapped in that it has exceeded its carrying capacity … Meanwhile, slaughter is ascribed to human rights violations, and the even more disturbing population pressure of demographic entrapment is conveniently forgotten. Demographic entrapment is so … disturbing that orthodox demography, public health, and UN agencies, particularly UNICEF, maintain a political correctness so correct that the entrapment is never mentioned… Maurice King, MD. From AJPH, July 1996
Factors associated with the genocide • Related to resource scarcity • Not related to resource scarcity
Related to Resource Scarcity • Popular discontent due to food scarcity • Gain from previous Tutsi “pogroms” • Fear of losing land to invading army • Joblessness
Rwanda population, 1900-2000 Source: US Census Bureau
Average land holding 1960s-1990s Source: Uvin, 1996
Food Production per Capita 1961-1993 Source: FAO, 1994
Over-population Resource scarcity Popular discontent Desire Ability Permission
Population density Source: PRB
Population density Source: PRB
Not Related to Resource Scarcity • Falling commodity prices • Popular discontent due to mismanagement • Elite worried about losing power • Long tradition of social division • Genocidal ideology • Effective propaganda and media • Highly disciplined state machinery • Lack of filial bonds: state vs. tribe • International inaction
Coffee Earnings, 1985-1993 Source: FAO, 1994
Unfavorable terms of trade / structural adjustment Over-population Arusha Steady arms supply Rebel attack International Inaction Resource scarcity Corruption Highly organized state Social divisions Popular discontent Elite insecurity Lack of filial bonds Effective media Desire Ability Permission
If population is so important Source: PRB
Outline • Population and fragility • Fragility and health • Health and fragility • Missions, health, and fragility
How fragility affects health • Security • Policies • Motivation • Training • Management • Sustainability • Communities • Responsibility
Outline • Population and fragility • Fragility and health • Health and fragility • Missions, health, and fragility
How health affects fragility • No services is a big part of fragility
How health affects fragility • No services is a big part of fragility • Good services legitimize governments
How health affects fragility • No services is a big part of fragility • Good services legitimize governments • Health is entry point for building systems
South Sudan example • Good human resource management • Good information system • Simple tools • Scaleable • Adapted to local environment
How health affects fragility • No services is a big part of fragility • Good services legitimize governments • Health is entry point for building systems • Systems may induce more responsibility
How health affects fragility • No services is a big part of fragility • Good services legitimize governments • Health is entry point for building systems • Systems may induce more responsibility • Community work strengthens communities
Key quality indicatorsCommunity distributors, South Sudan n = 96 supervision reports
Can Health Programs Help? a a • Poor information • Weak human resources • Weak absorptive capacity • Uncertain future • Unpredictable external support • Recidivism • Need to address immediate needs • Need to show peace dividend a x x x a a
Can Health Programs Help? • Enhance stability • Improve security • Encourage reform • Increase capacity in key areas • Address sources of fragility • Seek short-term impact & long-term reform • Establish measurement systems a a a a
Institutional Indicators from Health • Utilization rate • Reported supervisions / health area / month • % community workers reporting • % stock out for key drugs
Outline • Population and fragility • Fragility and health • Health and fragility • Missions, health, and fragility
Health, Fragility, and Missions • Missions are concerned about fragility • Missions care about health status • What do missions do that helps? • What do missions do that doesn’t help?
Health, Fragility, and NGOs • Field-based • Innovative • Collaborative • Coordinated • Think of scale-up • Expensive • Short term • Small scale • Not audited
Things that don’t help • Frequent strategic redesign • Process of strategic redesign • Little field presence • Concentrating resources • Lack of DC – Mission coordination • Some regulations – drugs, salaries • Short-term funding
Things that do help • Ambitious programs designed for scale • Coordination of grantees • Coordinating with other donors • Grantee – Government mediation • Inter-sector synergy • Willingness to support systems • Long-term funding